Thyroid Cancer
21.03.2025
THYROID CANCER DIAGNOSIS AND TREATMENT
Thyroid cancer is a type of cancer that starts in the thyroid gland. The thyroid gland is a butterfly-shaped gland located in the front of the neck and produces hormones that regulate metabolism. Thyroid cancer is generally a slow-growing type of cancer and can be treated when diagnosed early. However, some types of thyroid cancer can be more aggressive and spread quickly. The importance of this type of cancer is that it can be controlled with early diagnosis and treatment. When detected in the early stages, successful results can be achieved with surgery and other treatment methods. Therefore, it is important to consult a doctor immediately if any change or irregularity is felt in the thyroid gland. Thyroid cancer is more common, especially in women, and is usually diagnosed between the ages of 30 and 60. With early diagnosis and correct treatment, many people can overcome this disease and continue their normal lives.
WHAT ARE THE RISK FACTORS?
There are several risk factors that may contribute to the development of thyroid cancer. These factors do not mean that everyone will get thyroid cancer, but the presence of these factors may increase the risk of developing the disease. Thyroid cancer risk factors include:
Gender and Age: Thyroid cancer is more common in women. Additionally, most cases of thyroid cancer are diagnosed between the ages of 30 and 60.
Family History and Genetic Conditions: Thyroid cancer may show familial transmission. Some genetic conditions, such as multiple endocrine neoplasia type 2 (MEN 2), may increase the risk of thyroid cancer.
Exposure to Radiation: Radiation therapy to the head or neck area during childhood may increase the risk of thyroid cancer.
Thyroid Diseases: Some thyroid diseases, especially thyroid nodules or abnormal enlargement of the thyroid gland (goiter), can increase the risk of cancer.
Iodine Deficiency: Not getting enough iodine in the diet may increase the risk of thyroid diseases and therefore thyroid cancer.
Nutrition and Lifestyle: Poor or unbalanced diet and general lifestyle factors can also affect thyroid health.
Sex Hormones and Reproductive History: Female hormones and reproductive history, especially early menstruation or late menopause, can affect the risk of thyroid cancer.
Each of these factors may increase the risk of thyroid cancer to different degrees. However, the presence of risk factors does not necessarily mean that a person will get thyroid cancer. Adopting a healthy lifestyle and regular health checks can play an important role in reducing the risk.
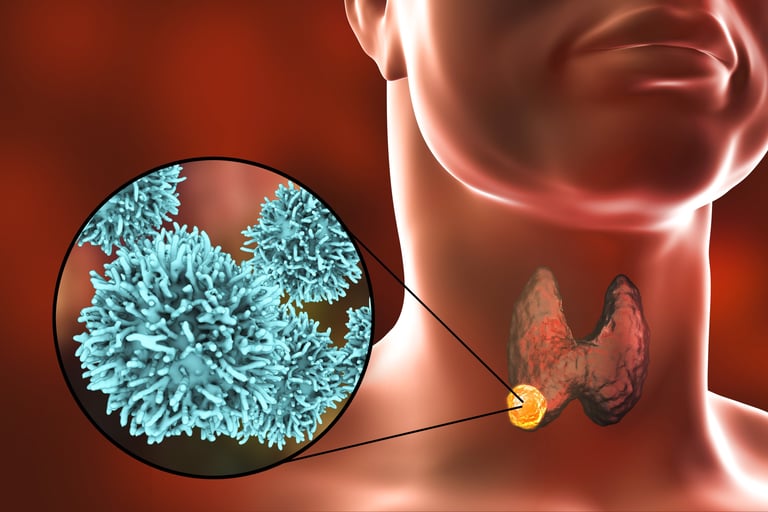
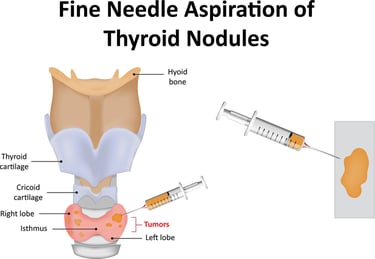
Image 1: Thyroid cancer is diagnosed by ultrasound-guided thyroid biopsy.
HOW IT OCCURS ?
The mechanisms of development of thyroid cancer are complex and diverse. Essentially, mutations or genetic changes in the DNA in thyroid cells cause the cells to grow and multiply in an uncontrolled and abnormal way. These mutations may alter the activity of oncogenes or tumor suppressor genes that prevent the death of cells, accelerate cell division, or allow cells to spread outside the thyroid gland. Radiation exposure, especially at young ages, can lead to DNA damage and such mutations, one of the best-known triggers of thyroid cancer. Additionally, hereditary factors such as some genetic syndromes and family history may also contribute to the development of thyroid cancer. The exact cause of mutations or genetic changes in all cases of thyroid cancer is not always clear. Thyroid cancer can be divided into several subtypes according to the degree of differentiation of the cells and the type of genetic changes, resulting in diversity of treatment approaches and prognosis.
WHAT ARE THE SYMPTOMS?
Signs and symptoms of thyroid cancer may sometimes not be obvious, but some common signs include:
Swelling or Mass in the Neck Area: Any swelling, node, or mass noticed in the thyroid gland or neck area is the most common symptom of thyroid cancer.
Hoarseness and Speech Changes: Thyroid cancer can cause hoarseness or changes in speech because it is close to the vocal cords.
Difficulty in Swallowing: A growing mass in the neck may cause difficulty in swallowing.
Difficulty Breathing: A large mass can put pressure on the airways, causing difficulty breathing.
Sore throat: Constant or recurring sore throat may be a sign of thyroid cancer.
Cough: A persistent cough, especially if accompanied by bloody sputum, is a symptom to be aware of.
These symptoms do not always indicate thyroid cancer and may be caused by other health conditions. But if you have any of these symptoms, especially if they last longer than a few weeks, it's important to consult a doctor. Early diagnosis is critical for the treatability of thyroid cancer.
HOW IS IT DIAGNOSED?
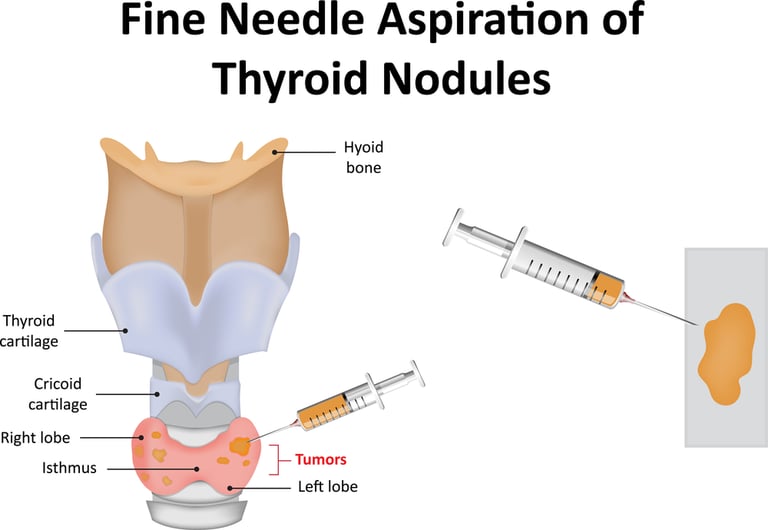
Thyroid cancer is diagnosed with a series of tests and films. The first step is usually a physical examination for a mass felt in the neck or other symptoms. The doctor examines the thyroid gland and lymph nodes in the neck area to look for any abnormalities. If there is a suspicious situation, imaging tests such as ultrasonography are used. Ultrasound is effective for evaluating the size, structure, and relationship of nodules or masses in the thyroid gland to surrounding tissues. Fine needle aspiration biopsy may be performed for more detailed information; In this process, cell samples are taken from the mass using a thin needle and examined under a microscope. Additionally, thyroid functions are evaluated with blood tests. More advanced imaging tests such as computed tomography (CT) or magnetic resonance imaging (MRI) may also be used if necessary. The combination of these tests is important to determine the presence and stage of thyroid cancer and helps create the appropriate treatment plan.
WHAT ARE THE PATHOLOGICAL TYPES?
Thyroid cancer is divided into several pathological types, which can arise from different cell types and each have their own unique characteristics and treatment approaches.
The most common types of thyroid cancer are:
Papillary Thyroid Cancer: It accounts for approximately 80% of thyroid cancer cases. It is generally a slow-growing type of cancer and usually has a good prognosis. It usually spreads to the lymph nodes.
Follicular Thyroid Cancer: It is the second most common type after papillary thyroid cancer. It is usually seen in middle-aged and elderly individuals. Follicular cancer can grow slightly faster than papillary cancer and can sometimes spread through the blood to distant organs, especially the lungs and bones.
Medullary Thyroid Cancer: It constitutes approximately 2-4% of thyroid cancers. It usually originates from the parafollicular C cells of the thyroid. This type of cancer may be related to MEN 2 (Multiple Endocrine Neoplasia type 2) syndrome and may involve a genetic component.
Anaplastic Thyroid Cancer: It is the most aggressive and deadliest type of thyroid cancer, but it is also the rarest. It grows and spreads rapidly, usually seen in the elderly. Anaplastic thyroid cancer is often resistant to treatment.
Each type of thyroid cancer looks different under the microscope and has different genetic and molecular characteristics. These features play an important role in determining how cancer is treated. Diagnosis is usually made by fine needle aspiration biopsy and subsequent pathological examination. This examination helps determine the type of cancer and its genetic characteristics, together with genetic testing when necessary. Some receptors and molecular targets are of critical importance in the treatment of thyroid cancer and in determining the course of the disease. Primarily for papillary and medullary thyroid cancers, tyrosine kinase inhibitors (TKIs) are an important treatment target. These receptors act on key signaling pathways that regulate cell growth and spread. RET and BRAF gene mutations are also of particular importance; RET mutations are frequently seen in medullary thyroid cancer, and BRAF mutations are frequently seen in papillary thyroid cancer, and these mutations may determine the aggressiveness of the cancer and its response to treatment. In medullary thyroid cancer, calcitonin and carcinoembryonic antigen (CEA) levels are taken into consideration in monitoring the disease and evaluating the response to treatment. Additionally, the presence and effect of estrogen and progesterone receptors in some thyroid cancers are being investigated, especially in female patients. Identification of these molecular targets and receptors is done through genetic and molecular testing, enabling the development of personalized treatment approaches based on the type of cancer and the individual genetic characteristics of the patient. These approaches enable more effective outcomes for patients by optimizing treatment options.
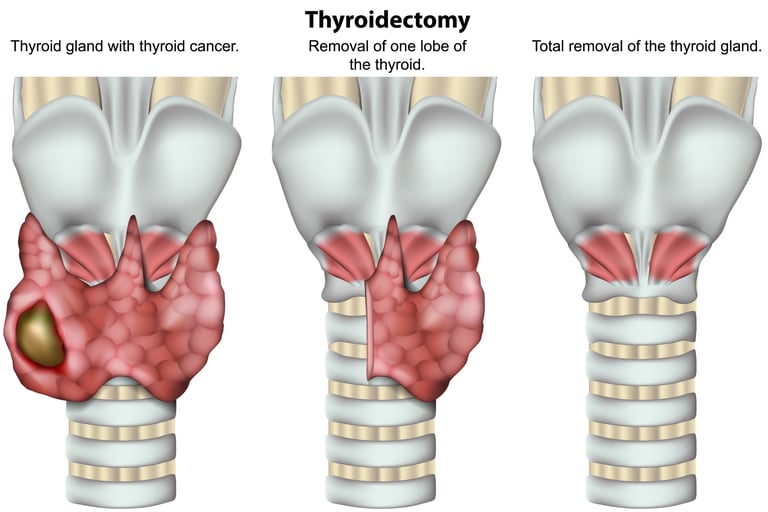
Image 2: The main treatment for thyroid cancer is surgery. All or almost all of the thyroid gland can be removed.
HOW IS TUMOR STAGING DONE?
Tumor staging in thyroid cancer is a system used to determine the extent of cancer spread and the patient's prognosis. This staging is usually based on the following criteria:
Tumor Size and Location (T): The size and location of the tumor in the thyroid gland is evaluated. It is divided into four categories: T1, T2, T3, and T4, where T1 represents the smallest and T4 represents the largest or most invasive tumors.
Spread to Lymph Nodes (N): It is examined whether the cancer has spread to the lymph nodes in the neck area. N0 means no lymph node spread; N1 indicates spread to lymph nodes.
Distant Metastasis (M): It is determined whether the cancer has spread to other parts of the body, such as the lungs or bones. M0 means no distant metastasis; M1 indicates the presence of metastasis.
The staging system is usually done using the TNM system recommended by the American Cancer Society. In this system, the general stage of the cancer is determined by combining the T, N and M categories. Thyroid cancer is divided into four main stages:
Stage I and II: They generally represent smaller tumors and limited spread. In these stages, the course of the disease is generally good.
Stage III: It includes larger tumors or conditions with regional spread.
Stage IV: It represents tumors that have distant metastasis or are very aggressive, and the prognosis is less favorable.
Thyroid cancer staging may also vary depending on the patient's age, histological type of tumor, and other factors. Staging plays an important role in treatment planning and prognosis prediction.
HOW IS TREATMENT DONE ACCORDING TO STAGES?
Treatment of thyroid cancer according to its stages is determined by taking into account the type and stage of the cancer, the general health status of the patient, and their preferences. Different treatment approaches can be applied at different stages:
Stage I and II (Early Stage):
Surgery: Partial (lobectomy) or complete (total thyroidectomy) removal of the thyroid gland is the most common treatment method.
Radioactive Iodine Therapy (RAI): Can be used to destroy remaining thyroid cells after surgery and clear microscopic cancer cells.
Thyroid Hormone Therapy: Thyroid hormone replacement therapy is used to keep thyroid hormone levels normal and ensure that TSH (Thyroid Stimulating Hormone) is kept low, which can inhibit the growth of cancer cells.
Stage III (Locally Advanced Stage):
Surgery: In most cases, total thyroidectomy and removal of affected lymph nodes is recommended.
Radioactive Iodine Therapy: It is widely used in locally advanced disease.
Radiation Therapy: May be required in some cases for local control.
Thyroid Hormone Therapy: Applied after surgery and RAI treatment.
Stage IV (Metastatic Stage):
Surgery: May be performed in selected cases to improve quality of life and reduce symptoms.
Radioactive Iodine Treatment: May be effective in metastatic disease, but may not be effective in all cases.
Radiation Therapy: May help control metastases.
Tyrosine Kinase Inhibitors (TKI): Used especially in RAI-resistant or advanced disease.
Targeted Therapy and Immunotherapy: Can be applied depending on genetic mutations or other molecular targets.
At each stage of thyroid cancer, a multidisciplinary approach is often preferred to create the most effective treatment plan. Multidisciplinary work involves endocrinologists, oncologists, radiation oncologists, and surgeons working together. The patient's active role in the treatment process and regular follow-ups are also important for the success of the treatment.
Image 3: In individuals with thyroid cancer, thyroid hormone therapy may need to be adjusted and smart drug therapies may need to be used after surgery.


WHAT ARE THE DRUGS USED IN TREATMENT?
Treatment options used in thyroid cancer vary depending on the type and stage of the cancer. The main treatment methods used are:
Chemotherapy drugs: Chemotherapy is not often used to treat thyroid cancer, but may be used in some advanced or treatment-resistant cases. Chemotherapeutic agents may include doxorubicin and cisplatin.
Hormonal Drugs: Levothyroxine (T4): Used for thyroid hormone replacement therapy. It is used to lower TSH levels after total thyroidectomy and thus prevent the growth of cancer cells.
Smart Drug Therapies (Targeted Therapies): Tyrosine Kinase Inhibitors (TKI): Used in papillary and medullary thyroid cancers. These drugs attack specific molecular targets that help cancer cells grow and spread. Examples include sorafenib, lenvatinib, and vandetanib. RET Inhibitors are drugs that target RET mutations in medullary thyroid cancer. For example, selpercatinib and pralsetinib.
Immunotherapies: Immunotherapies are among the promising treatment options, especially in advanced or metastatic thyroid cancer. These treatments are designed to make the immune system more effective against cancer cells. PD-1 inhibitors such as pembrolizumab are in this group.
Each treatment option is personalized based on the type of cancer, the patient's overall health, previous responses to treatment, and other factors. Treatment planning should be done by a multidisciplinary team, taking into account the patient's needs and the potential benefits and risks of treatment.
HOW SHOULD FOLLOW-UP BE CARRIED OUT AFTER RECOVERY?
Follow-up after recovery from thyroid cancer is critical to detect early disease recurrence and monitor long-term health status. Follow-up usually begins with regular adjustments of thyroid hormone replacement therapy and thyroid function tests. These tests monitor Thyroid Stimulating Hormone (TSH) and thyroxine (T4) levels. Additionally, regular physical examinations and neck ultrasonography are performed to detect any abnormalities or a reoccurring mass in the neck area. In some cases, especially in high-risk patients, further imaging tests such as a whole-body radioactive iodine scan or PET/CT scan may be required at regular intervals. It is also recommended to monitor calcitonin and carcinoembryonic antigen (CEA) levels for patients with medullary thyroid cancer. Patients themselves should also report any new symptoms or changes to their doctors. This follow-up plan should be individualized on a patient-by-patient basis and adjusted according to the patient's age, stage of cancer, and type of treatment. More frequent follow-up is recommended, especially during the first five years, because the risk of recurrence is higher during this time.
Legal Information
The brand name ''Onkoloji Doktorum'' has been registered by the Turkish Patent and Trademark Office.
All content on this site is for informational purposes for patients receiving cancer treatment in Türkiye. Consult your doctor for treatment planning.
All content on the site is translated from Turkish. Translation errors may be present. An oncology physician should be consulted for incomprehensible information.
All articles and images used on our website are licensed and protected by DMCA. Unauthorized use or copying is prohibited.
Contact
Assoc. Prof. Dr. İzzet Doğan
Internal Medicine and Medical Oncology Specialist
Acıbadem Healthcare Group
Atakent ve Bakırköy Hospitals
Call for an Appointment: +90 444 55 44
Acıbadem Atakent Hospital
Telephone: +90 212 404 44 44
Acıbadem Bakırköy Hospital
Telephone: +90 212 414 44 44