Basal Cell Carcinoma of the Skin
21.03.2025
DIAGNOSIS AND TREATMENT OF SKIN BASAL CELL CARCINOMA
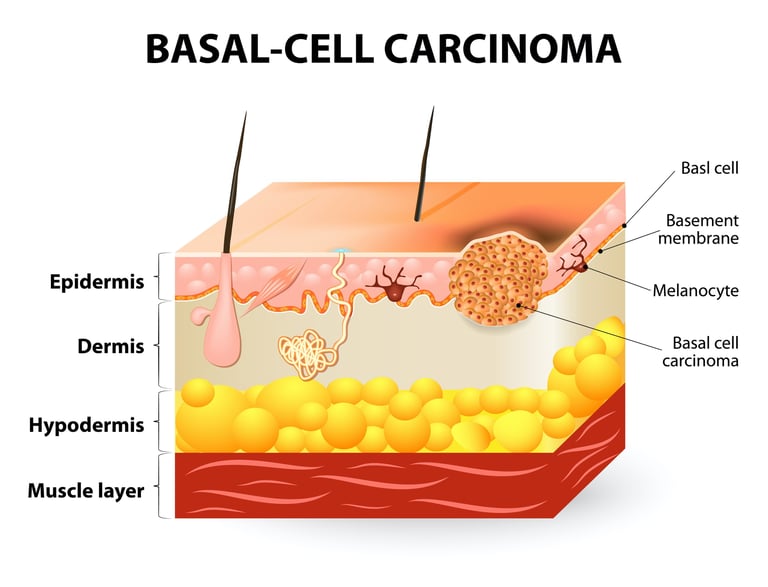
Cutaneous basal cell carcinoma (BCC) is a type of skin cancer that originates from the basal cells located at the bottom of the upper layer of the skin, called the epidermis. BCC is generally a slow-growing type and rarely tends to metastasize to other body parts. However, if left untreated, it can cause damage to local tissues. It is frequently seen on the skin, especially in areas exposed to the sun, such as the face, neck, hands and arms. Early diagnosis and treatment of skin basal cell carcinoma is extremely important because it can form larger lesions in later stages. It is important that this type of skin cancer can be prevented or diagnosed early by taking adequate protective measures and regular skin examinations. Treatment options for cutaneous BCC include surgical excision, radiotherapy, cryotherapy (cold therapy) and some medications. Skin BCC is a type of cancer that can be successfully treated with early diagnosis and appropriate treatment.
WHAT ARE THE RISK FACTORS?
There are various risk factors that can lead to the development of skin basal cell tumor (BCC). These factors may include:
Prolonged Sun Exposure: Long-term exposure to the sun and sunburn increase the risk of skin cancer. People with light skin, blond hair or blue eyes are especially at greater risk.
Age: BCC risk increases with age. As we age, skin cells may become more susceptible to sun damage.
Skin Type: People who have fair skin, are exposed to the sun frequently, or are more sensitive to the sun are at higher risk.
Family History: Family history may increase the risk of skin cancer. If family members have a history of BCC or other types of skin cancer, an individual's risk may be increased.
Ultraviolet (UV) Rays: Solarium use or work-related UV exposure may increase the risk of BCC.
Skin Damage:Burns, scars, or other skin damage may increase the risk of BCC.
Radiation Exposure: The risk of BCC may increase in people who have been exposed to radiation for radiotherapy or other reasons.
Smoking and Alcohol Use:Smoking and excessive alcohol consumption may increase the risk of skin cancer.
Immune System Weakness: People with weak immune systems may be at risk of BCC. People who receive organ transplants or use medications that suppress the immune system are at risk.
Xeroderma Pigmentosum (XP): XP, a rare genetic disorder, may increase the risk of skin cancer when exposed to sunlight.
These risk factors can affect the likelihood of developing BCC, but not everyone can get skin cancer even if they don't have these factors. Therefore, taking precautions such as sun protection and regular skin exams are important in reducing the risk of BCC.
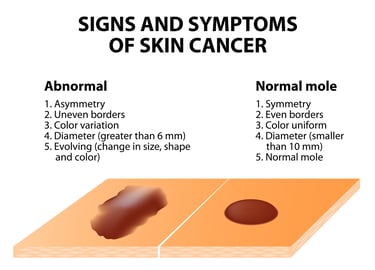
Image 1: Suspicious skin lesions should be monitored for cancer development.
HOW IT OCCURS ?
Skin basal cell carcinoma (BCC) development mechanisms usually occur due to long-term sun exposure. Ultraviolet (UV) rays of sunlight can cause DNA damage in skin cells. This DNA damage causes uncontrolled proliferation of normal cells, especially in basal cells. This damage to the DNA of skin cells triggers the onset of basal cell carcinoma. Additionally, factors such as genetic predisposition of the skin, family history and weakness of the immune system may also increase the risk of BCC. In conclusion, the combination of sun exposure and genetic factors contribute to the development of cutaneous BCC and constitute the basic mechanisms of this type of cancer.
WHAT ARE THE SYMPTOMS?
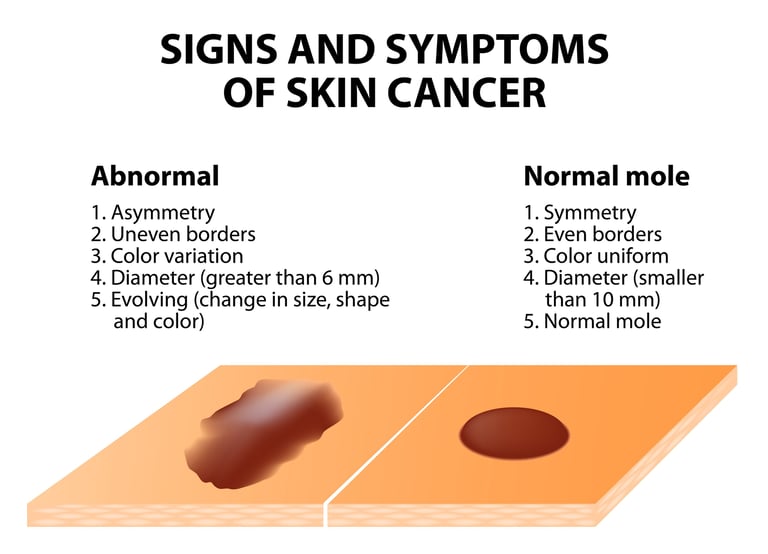
Signs and symptoms of skin basal cell carcinoma (BCC) may include:
Raised or Flat Lesions: BCC usually begins as raised or flat, shiny or pink colored lesions on the skin surface. These lesions may grow larger over time.
Wounds and Ulcerations: In advanced stages of BCC, lesions may develop into sores or ulcerations. These wounds often lead to bleeding, crusting, and scabs.
Shiny Edges: Shiny or pearl-white colored edges may be seen around the lesions.
Bleeding and Crusting: Certain types of BCC may occasionally bleed, crust, or ulcerate superficially.
Similar Skin Changes: BCC can look similar to other similar-looking skin problems, so it should be examined by a dermatologist for a correct diagnosis.
Itching or Pain: In some cases of BCC, the lesions may cause itching or mild pain.
It should be noted that BCC usually grows slowly and rarely metastasizes, but if left untreated, it can damage local tissues. Therefore, any abnormal changes or symptoms on the skin should be taken into consideration. In case of any doubt, consulting a dermatologist is critical for early diagnosis and treatment.
HOW IS IT DIAGNOSED?
The diagnosis of skin basal cell tumor (BCC) is usually made by a dermatologist through physical examination. During the examination, abnormal lesions and similar changes on the skin surface are examined. When a suspicious lesion is detected, the dermatologist usually performs a biopsy. Biopsy involves taking a small tissue sample of the lesion and this sample is sent for pathological examination. Pathological examination confirms that the lesion is definitely BCC and determines its type. The diagnosis of BCC is made based on the appearance of the lesion, biopsy results, and the patient's medical history. This diagnostic process helps diagnose the disease early and create an appropriate treatment plan.
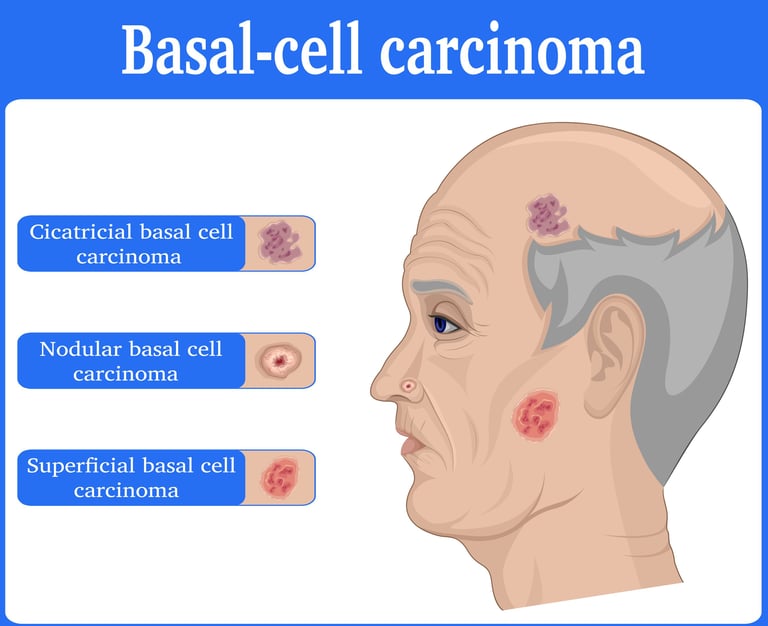
WHAT ARE THE PATHOLOGICAL TYPES?
There are different pathological types of cutaneous basal cell carcinoma (BCC), and each provides information about the cellular structure and behavior of the tumor. The most common pathological types are:
Superficial BCC: This type usually appears on the upper layer of the skin surface (epidermis) and appears as non-swelling, reddish or pink colored lesions.
Nodular BCC: This type of BCC has a more rounded, raised appearance and usually grows slowly. There may be ulceration (wound) in the center.
Sclerodermiform BCC: This type is one that causes less distinct borders and hardening of the skin. It is often more difficult to diagnose than other types.
Ulcerative BCC: This type of BCC appears as lesions with ulcerations (wounds) on the surface and often crusting in the middle.
Superficial Erosive BCC: This type is characterized by erosive lesions that appear irregularly on the skin surface, usually at multiple points.
Basosquamous Cell Carcinoma: This type shows both basal cell and squamous cell features. It is considered a more aggressive type and the treatment approach may vary.
Each pathological type plays an important role in determining treatment options and assessing prognosis. Therefore, the pathological type of the tumor should be taken into account by doctors and the patient's treatment plan should be created accordingly. Evaluation of specific receptors or markers in cases of cutaneous basal cell carcinoma (BCC) is typically less common than in other types of cancer. However, in some specific subtypes of BCC or treatment-resistant cases, specific receptors and proteins can be examined. In particular, Hedgehog signaling pathway receptors (e.g., Smoothened) and activation of the Sonic Hedgehog (SHH) gene play an important role in the occurrence of BCC. Therefore, these receptors and gene activation may be important in determining and monitoring some treatment methods. However, the diagnosis of BCC is usually made by histopathological examinations and evaluation of a skin biopsy, and routine testing of receptors or markers is not required. In all cases, the patient's treatment and follow-up plan should be determined by skin cancer specialists based on the patient's specific situation.
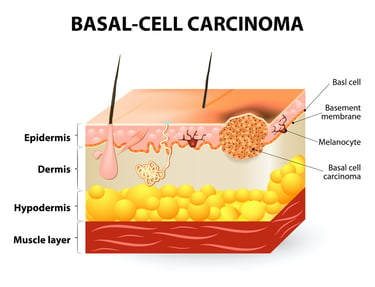
Image 2: BCC can develop in elderly individuals on the face that has been exposed to UV rays for a long time.
HOW IS TUMOR STAGING DONE
Skin basal cell carcinoma (BCC) staging is used to determine the extent of spread of the cancer and its spread on the skin. The staging system recommended by the American Joint Committee on Cancer (AJCC), developed by the American Cancer Society, defines the following stages of BCC:
Evre 0 (Tis)This stage, called carcinoma in situ, indicates that the cancer cells are limited to the surface epidermis layer and have not spread to the surrounding tissues.
Stage I: The cancer has spread below the surface but has not yet spread to nearby lymph nodes or other organs. The size and depth of the tumor are evaluated at this stage.
Stage II: The tumor has spread deeper, but still has not spread to the lymph nodes or other organs.
Stage III: Cancer has spread to lymph nodes or nearby tissues, but has still not reached more distant organs.
Stage IV: Cancer has spread to distant organs or different parts of the body. This stage is called metastatic cancer and usually indicates a more serious prognosis.
Tumor staging is based on the results of the patient's physical examination, biopsy results, imaging studies (for example, computed tomography or magnetic resonance imaging), and sentinel lymph node biopsies to determine the status of the lymph nodes. This information helps assess the spread of cancer and helps determine appropriate treatment options.
HOW IS TREATMENT DONE ACCORDING TO STAGES?
Treatment for skin basal cell carcinoma (BCC) may vary depending on the stage and type of cancer and the patient's overall health. Treatment approaches according to stages:
Stage 0 (Tis) and Stage I: BCC in these stages is usually limited to the skin surface. Treatment is usually done by surgical excision. The entire lesion is removed, usually along with the healthy tissue under the skin.
Stage II: Stage II BCC may have spread deep into the skin layers, but has not yet spread to the lymph nodes or other organs. Treatment is again done by surgical excision, and it is important to check the tissues around and underneath the deeply removed tumor.
Stage III: At this stage, BCC has spread to lymph nodes or nearby tissues. Treatment may include surgical excision as well as removal of lymph nodes. Radiotherapy can also be used to treat BCC at this stage.
Stage IV: Stage IV BCC has metastasized to distant organs or different parts of the body. At this stage, surgical treatment options are limited and systemic treatments, that is, drug treatments such as chemotherapy, targeted drugs or immunotherapy, are more commonly used.
The treatment plan should be determined according to the specific situation of each patient. Specialists such as dermatologists, oncologists and surgeons determine the most appropriate treatment options by evaluating the patient's cancer stage and general health condition. In addition, it is important to take regular follow-up and skin protection measures after treatment, because there is a risk of recurrence of BCC and early diagnosis can increase the success of treatment.
Image 3: The primary treatment for BCC is surgery. In cases where surgery is not possible, radiotherapy or smart drug treatments can be used.


WHAT ARE THE DRUGS USED IN TREATMENT?
Treatment options used in the treatment of skin basal cell carcinoma (BCC) do not include chemotherapy, hormonal drugs, targeted smart drugs and immunotherapy. This is because BCC is generally a slow-growing type of cancer and other treatment methods are more likely to be effective. However, in more aggressive or treatment-resistant cases of BCC, some medications or methods may be used:
Chemotherapy: BCC does not usually respond to chemotherapy, so this treatment method is used in a limited way and other treatment options are often preferred.
Smart Drugs (Targeted Therapies): In some specific cases of BCC, especially fast-growing or treatment-resistant tumors, targeted drugs may be used. For example, drugs that target the Hedgehog signaling pathway, such as vismodegib or sonidegib, fall into this category.
Immunotherapy: Immunotherapy for BCC is often used in cases of metastatic or advanced BCC. Immunotherapy drugs, such as pembrolizumab and nivolumab, stimulate the immune system to attack cancer cells.
An important point to remember is that each patient's condition may be different, and the treatment plan is personalized based on the patient's stage, species, genetic characteristics, and health status. Therefore, collaboration with a dermatologist or oncologist should be sought to determine the most appropriate options for treating BCC.
HOW SHOULD FOLLOW-UP BE CARRIED OUT AFTER RECOVERY?
Once skin basal cell carcinoma (BCC) treatment is successfully completed, post-recovery follow-up is important. The monitoring program aims to detect early recurrence or metastasis of cancer. Therefore, patients should be regularly monitored by a dermatologist or oncologist. The monitoring period is determined by the person's type of BCC, its stage, and response to treatment. Typically, during follow-up visits, skin examinations are performed, the recurrence of lesions or the formation of new lesions is observed, lymph nodes are checked, and imaging studies or biopsies may be performed if necessary. Patients should also maintain sun protection measures and promptly report any suspicious skin changes to their physician. Early diagnosis and regular follow-up can improve the quality of life after BCC treatment and reduce the risk of recurrence.
Legal Information
The brand name ''Onkoloji Doktorum'' has been registered by the Turkish Patent and Trademark Office.
All content on this site is for informational purposes for patients receiving cancer treatment in Türkiye. Consult your doctor for treatment planning.
All content on the site is translated from Turkish. Translation errors may be present. An oncology physician should be consulted for incomprehensible information.
All articles and images used on our website are licensed and protected by DMCA. Unauthorized use or copying is prohibited.
Contact
Assoc. Prof. Dr. İzzet Doğan
Internal Medicine and Medical Oncology Specialist
Acıbadem Healthcare Group
Atakent ve Bakırköy Hospitals
Call for an Appointment: +90 444 55 44
Acıbadem Atakent Hospital
Telephone: +90 212 404 44 44
Acıbadem Bakırköy Hospital
Telephone: +90 212 414 44 44