Ovarian Cancer
21.03.2025
OVARIAN CANCER DIAGNOSIS AND TREATMENT

Ovarian cancer is a type of cancer that begins in the ovaries of women. Ovarian cancer usually has no symptoms in the early stages, so it can be difficult to diagnose. When symptoms appear, they may include abdominal bloating, digestive problems, rapid weight loss, and pelvic pain. Ovarian cancer can be quite dangerous if left untreated, especially in advanced stages. Regular gynecological examinations and awareness of risk factors are critical in the early diagnosis of this cancer. When diagnosed early, successful results can be achieved with treatment methods such as surgery and chemotherapy. Therefore, it is of great importance to raise awareness about ovarian cancer and not to neglect regular health checks.
WHAT ARE THE RISK FACTORS?
Ovarian cancer risk factors include various factors that may increase the likelihood of developing this type of cancer. Although each of these risk factors is not a definitive cause for the development of cancer, their presence may increase the risk.
Known risk factors of ovarian cancer are:
Age: Ovarian cancer is generally more common in women aged 50 and over, but it can occur at any age.
Genetic Factors: Having a family history of ovarian, breast, uterine or colon cancer may increase the risk. In particular, BRCA1 and BRCA2 gene mutations significantly increase the risk of ovarian cancer.
Cancer History: The risk of ovarian cancer is higher in women with a history of breast cancer or other gynecological cancers.
Menstruation Date: Early onset of menstruation (before age 12) and/or late menopause (after age 51) may increase the risk of ovarian cancer.
Non-Birth or First Birth at a Late Age: Having never given birth or having your first birth after the age of 30 may increase the risk.
Hormone Therapy: Postmenopausal hormone replacement therapy (especially estrogen-only treatments) may increase the risk of ovarian cancer.
Infertility and Infertility Treatments: The risk may be slightly higher in women who have had infertility or infertility treatments.
Endometriosis: The risk of ovarian cancer may increase in women with endometriosis.
Obesity and Lifestyle Factors: High body mass index and unhealthy lifestyle choices may affect the risk of ovarian cancer.
Having one or more risk factors does not necessarily mean that you will develop ovarian cancer. Being aware of these risk factors and having regular health checks is important for early diagnosis and treatment. People with risk factors are recommended to discuss these risks and possible screening methods with their doctors.
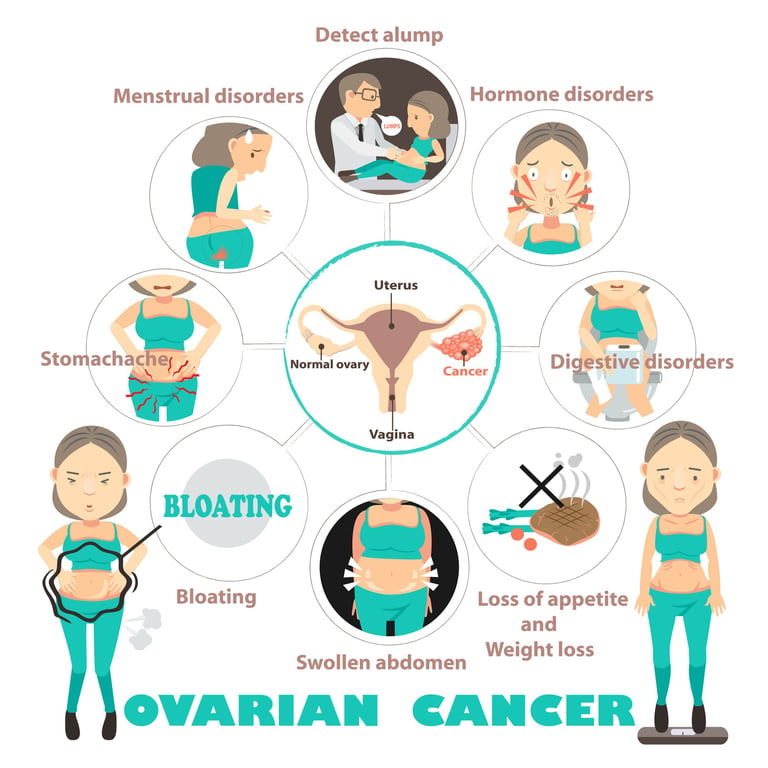
Image 1: Ovarian cancer can develop insidiously and manifest itself as abdominal swelling, digestive disorders and abdominal pain.
HOW DOES IT OCCUR?
Ovarian cancer develops when cells in the ovaries multiply uncontrollably and abnormally. This process usually begins as a result of DNA damage or genetic mutations. These changes in DNA disrupt the normal growth and death processes of cells, causing the cells to begin dividing and multiplying uncontrollably. Ovarian cancer usually begins in the epithelial cells of the ovaries (the cells that line the outer surface of the ovaries), but it can sometimes arise in other cell types of the ovaries. Some genetic factors, such as BRCA1 and BRCA2 gene mutations, increase the risk of developing ovarian cancer. This type of cancer starts from the ovaries and can spread to the abdominal cavity and other organs. While it usually does not cause symptoms in the early stages, as it progresses, it can cause symptoms such as abdominal bloating, pain and digestive problems. The development of ovarian cancer is a complex process and progresses through the interaction of many different factors. That's why regular screenings and awareness of risk factors are critical for early diagnosis.
WHAT ARE THE SYMPTOMS?
Ovarian cancer often does not cause symptoms, especially in the early stages, but some symptoms may appear in the later stages. Although these symptoms are nonspecific, it is important to consult a doctor when suspected.
Common symptoms of ovarian cancer include:
Feeling of Swelling or Fullness in the Abdominal Area: As the cancer grows, swelling or fullness may be felt in the abdominal area.
Pelvic or Abdominal Pain: Ovarian cancer often causes pain in the pelvic area or lower abdomen.
Digestive Problems: Digestive problems such as loss of appetite, nausea, gas or constipation may occur.
Need to Urinate Frequently: Ovarian cancer can put pressure on the bladder, causing the need to urinate frequently.
Rapid Weight Loss or Gain: There may be sudden weight loss or weight gain.
Menstrual Irregularities: Changes in menstrual cycles or abnormal bleeding may be observed.
Tiredness: A general feeling of weakness and fatigue is common.
Each of these symptoms can be caused by other health problems, so the presence of these symptoms does not necessarily mean that you have ovarian cancer. However, if any of these symptoms persist for a long time or become severe, it is important to consult a healthcare professional. Early diagnosis can make a big difference in the treatment of ovarian cancer
HOW IS IT DIAGNOSED?
Ovarian cancer is usually diagnosed through a series of tests and procedures. In a patient showing suspicious symptoms, the first step is usually to take a detailed medical history and physical examination, during which the doctor checks for any masses or abnormal fluid accumulation in the abdominal area. Pelvic exam, ultrasound, and a blood test called CA-125 are frequently used diagnostic methods. Pelvic ultrasound is used to see the structure of the ovaries and possible masses. The CA-125 test measures blood levels of a protein associated with cancer, but this test is not always accurate and may be high in other cases. If these tests strengthen the suspicion of cancer, surgical procedures called laparoscopy or laparotomy are usually performed for definitive diagnosis. During these procedures, the doctor may take tissue samples from the abdominal area and examine them under a microscope to confirm the presence of cancer cells. Imaging tests (CT, MRI) may also be used to determine the spread and stage of the cancer. The diagnosis of ovarian cancer is made with a multidisciplinary approach, based on the results of these tests and procedures, and each patient's situation is evaluated individually.
WHAT ARE THE PATHOLOGICAL TYPES?
Ovarian cancer is divided into several different pathological types according to its starting point and cellular structure. These types may affect the treatment and prognosis of cancer. The main pathological types of ovarian cancer are:
Epithelial Tumors: It accounts for approximately 90% of ovarian cancers. These tumors arise from the epithelial cells lining the outer surface of the ovaries. Epithelial ovarian cancers are divided into subtypes such as serous, mucous, endometrioid and clear cell tumors.
Germ Cell Tumors: These tumors arise from the egg-producing germ cells of the ovaries and usually occur in younger women. The most common types of germ cell tumors are dysgerminomas and non-germinomatous germ cell tumors.
Stromal Tumors: It originates from the supporting tissues (stroma) of the ovaries and accounts for a small percentage of ovarian cancers. These tumors usually produce hormones and are divided into types such as granulosa cell tumors, theca cell tumors, and Sertoli-Leydig cell tumors.
Metastatic Tumors: These are cancers that spread to the ovaries from other organs. For example, it is possible for stomach cancer (known as a Krukenberg tumor) or breast cancer to metastasize to the ovaries.
Each type of ovarian cancer exhibits different biological behaviors and responds to different treatment methods. Therefore, it is important to clearly understand the pathological type in order to determine the correct diagnosis and appropriate treatment plan. Pathological diagnosis is usually made by examining tissue samples taken during surgical intervention under a microscope.
In ovarian cancer, various receptors and molecular markers that play an important role in the treatment and prognosis of the disease are examined. The presence or absence of these receptors helps determine how well the cancer responds to certain treatments. The most important receptors include estrogen and progesterone receptors (ER and PR); the presence of these receptors may mean that it may respond to hormone therapy. Additionally, CA-125 levels are used to monitor the spread of cancer and evaluate treatment response. While Ki-67 indicates the growth rate and aggressiveness of the tumor, p53 tumor suppressor gene mutations and BRCA1/BRCA2 gene mutations can affect the biological behavior of cancer. Changes in components of the PI3K/AKT/mTOR pathway and other molecular markers such as microsatellite instability (MSI) may also predict response to specific treatments such as immunotherapy. Analysis of these receptors and markers allows the development of personalized approaches to the treatment of ovarian cancer and plays a critical role in creating treatment plans tailored to each patient's specific situation.
Image 2: Ovarian cancer treatment is performed with surgery, chemotherapy and smart drug treatments depending on the stage of the disease.
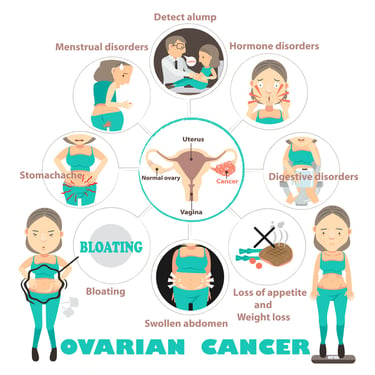
HOW IS TUMOR STAGING DONE?
Tumor staging in ovarian cancer is done to determine the extent of spread of the disease and how far it has progressed in the body. This staging is crucial for treatment planning and prognosis prediction. Ovarian cancer is usually staged using a system established by FIGO (International Federation of Gynecological Cancers). This staging system is as follows:
Stage I: Cancer is limited to the ovaries only.
Stage IA: The cancer is in a single ovary and the integrity of the capsule is intact.
Stage IB: Cancer is present in both ovaries, but the capsules are intact.
Stage IC: Cancer is present in one or both ovaries and the capsule has broken down or tumor cells have spread into the abdominal cavity during surgery.
Stage II:Cancer has spread to other tissues in the pelvic area.
Stage IIA: Cancer has spread to the uterus and/or fallopian tubes.
Stage IIB: Cancer has spread to other pelvic tissues.
Stage III: The cancer has spread outside the lower part of the abdominal cavity but has not penetrated into the liver.
Stage IIIA: Microscopically proven extra-abdominal spread.
Stage IIIB: Extra-abdominal tumors macroscopically smaller than 2 cm.
Stage IIIC: Extra-abdominal tumors larger than 2 cm and/or spread to lymph nodes.
Stage IV:Cancer has spread into the liver or other distant parts of the body.
Stage IVA: Cancer fluid contains cancer cells in the lining of the lung (pleural fluid).
Stage IVB: Cancer has spread to the liver or other distant parts of the body.
This staging is usually supported by pathological examination of samples taken by surgical intervention, imaging techniques such as computed tomography (CT) or magnetic resonance imaging (MRI), and biopsy if necessary. Staging results are used to determine treatment options and evaluate the patient's prognosis. Each stage shows different characteristics that indicate the spread and severity of cancer, and treatment strategies are determined accordingly.
HOW IS TREATMENT DONE ACCORDING TO STAGES?
Treatment for ovarian cancer varies depending on the stage of the cancer, the patient's general health and other individual factors. Below, I will summarize general treatment approaches according to the stages of ovarian cancer:
Stage I (Early Stage):
Surgery: Stage I ovarian cancer is usually treated with surgery. Surgery may involve removal of the cancerous ovary (oophorectomy) or both ovaries (bilateral oophorectomy), uterus (hysterectomy), and surrounding cancerous tissue.
Chemotherapy: In some cases, chemotherapy may be recommended after surgery, especially if the cancer is high-grade or there are complications such as capsule rupture during surgery.
Stages II and III (Locally Advanced Stage):
Surgery: In Stages II and III, surgery aims to remove as much of the tumor as possible (debulking surgery). Chemotherapy is recommended for the treatment of remaining microscopic disease after surgery.
Chemotherapy: Chemotherapy after surgery helps prevent or delay the return of cancer. Intraperitoneal chemotherapy may, in some cases, involve administering medication directly into the abdomen.
Stage IV (Metastatic Stage):
Surgery: In stage IV cancer, surgery may be intended to relieve symptoms (palliative surgery).
Chemotherapy: Systemic chemotherapy aims to control the spread of cancer to other parts of the body.
Targeted Therapies and Immunotherapy: Some patients may receive targeted therapies or immunotherapy depending on genetic mutations (for example, BRCA mutations) or molecular characteristics of the tumor.
At all stages, the response to treatment and the patient's condition are evaluated regularly. Treatment plans are personalized based on the patient's needs and preferences. Additionally, supportive care and palliative care services may be offered to improve patients' quality of life and manage treatment side effects. Significant advances have been made in the treatment of ovarian cancer in recent years, and new treatment options such as molecular targeted therapies and immunotherapy are being investigated. It is important for patients to discuss treatment options, risks, and benefits with their doctors in detail.
Image 3: Ovarian cancer treatment is managed by a multidisciplinary team consisting of gyneco-oncology and medical oncology doctors.


WHAT ARE THE DRUGS USED IN TREATMENT?
Treatment methods used in ovarian cancer include chemotherapy, hormonal drugs, targeted therapies (smart drugs) and immunotherapies. These treatment options vary depending on the type of cancer, its stage, and the patient's overall health. Here are the main treatment methods used in ovarian cancer:
Chemotherapy Drugs:
Platinum Based Agents: Cisplatin, carboplatin.
Taxanes: Paclitaxel, Docetaxel.
AntimetaboliteS: Gemsitabine.
Topoisomerase Inhibitors: Topotecan, irinotecan
Anthracyclines: Doxorubicin, Liposomal doxorubicin
Hormonal Treatments:
Aromatase Inhibitors: letrozole, anastrozole.
Gonadotropin Releasing Hormone (GnRH) Analogs: goserelin, leuprolide.
Targeted Therapies (Smart Drugs):
PARP Inhibitors: Olaparib, niraparib, rucaparib. It is especially used in patients with BRCA mutation.
Angiogenesis Inhibitors: Bevacizumab.
Drugs Targeting the PI3K/AKT/mTOR Pathway: Everolimus.
Immunotherapies:
PD-1/PD-L1 Inhibitors: For example, pembrolizumab, nivolumab.
CTLA-4 Inhibitors: For example, ipilimumab.
These treatment methods can be used alone or in combination, depending on the characteristics of the disease and the patient's health condition. The treatment plan is customized to the patient's needs and is usually managed by a multidisciplinary team. Additionally, new treatment options and clinical trials are constantly evolving in the treatment of ovarian cancer. It is important for patients to have open communication with their doctors about treatment options and possible side effects.
HOW SHOULD FOLLOW-UP BE CARRIED OUT AFTER RECOVERY?
Regular follow-up of patients during the recovery period after ovarian cancer treatment is extremely important because it is a critical step to detect early cancer recurrence and improve quality of life. Follow-up is usually done to evaluate the patient's response to treatment, possible side effects, and general health status. This process includes regular physical exams, usually every 3-6 months, pelvic exams, and blood tests of tumor markers such as CA-125. Imaging tests (for example, computed tomography or magnetic resonance imaging) may be repeated at intervals depending on the patient's condition and response to treatment. Post-treatment follow-up may also include supportive care services such as psychological support, nutritional counseling, and rehabilitation programs. Patients are advised to contact their healthcare provider immediately with any new symptoms or concerns. It is vital for patients to comply with regular follow-up programs in order to detect possible recurrence early and to make appropriate interventions in a timely manner. Post-treatment follow-up plans are customized to the patient's individual needs and can be adjusted based on the patient's health status.
Legal Information
The brand name ''Onkoloji Doktorum'' has been registered by the Turkish Patent and Trademark Office.
All content on this site is for informational purposes for patients receiving cancer treatment in Türkiye. Consult your doctor for treatment planning.
All content on the site is translated from Turkish. Translation errors may be present. An oncology physician should be consulted for incomprehensible information.
All articles and images used on our website are licensed and protected by DMCA. Unauthorized use or copying is prohibited.
Contact
Assoc. Prof. Dr. İzzet Doğan
Internal Medicine and Medical Oncology Specialist
Acıbadem Healthcare Group
Atakent ve Bakırköy Hospitals
Call for an Appointment: +90 444 55 44
Acıbadem Atakent Hospital
Telephone: +90 212 404 44 44
Acıbadem Bakırköy Hospital
Telephone: +90 212 414 44 44