Neuroendocrine Tumors
21.03.2025
NEUROENDOCRINE TUMOR DIAGNOSIS AND TREATMENT


Neuroendocrine tumors (NETs) are rare tumors that usually arise from hormone-producing endocrine cells. These cells can be found in various parts of the body and regulate various functions of the body through hormones. NETs are usually found in organs such as the pancreas, stomach, intestines, lung, and thymus. These tumors can grow slowly or rapidly, and some may secrete active hormones, causing a variety of symptoms. The importance of NETs is that they can often develop without obvious symptoms and are therefore often diagnosed late. When diagnosed early, NETs are usually treatable, but NETs in advanced stages or that have metastasized require a more challenging course of treatment. Treatment of NETs varies depending on the type of tumor, its location, rate of growth, and possible hormone production. Treatment methods include surgery, hormone therapy, radiotherapy, chemotherapy and targeted therapy options. Management of NETs can be complex and often requires a multidisciplinary approach. Therefore, collaboration between doctors from different specialties such as endocrinology, gastroenterology, oncology and radiology is important in the diagnosis and treatment of NETs.
WHAT ARE THE RISK FACTORS?
Neuroendocrine tumors (NETs) are rare types of cancer, and the exact risk factors that may contribute to the development of these tumors are not fully understood. However, some potential risk factors have been identified:
Genetic Factors: Some genetic syndromes may increase the risk of developing NETs. For example, conditions such as Multiple Endocrine Neoplasia type 1 (MEN1), von Hippel-Lindau syndrome, neurofibromatosis type 1 (NF1), and Tuberous Sclerosis may increase the risk of developing NETs.
Family History: People with a family history of NETs may have a higher risk of developing these tumors.
Age and Gender: Some types of NETs may be more common in certain age groups and genders.
Chronic Health Conditions: Long-term conditions that reduce stomach acid production, such as chronic atrophic gastritis or Zollinger-Ellison syndrome, may increase the risk of developing certain gastroenteropancreatic NETs.
Environmental Factors: Although there is no clear information on specific environmental factors that may play a role in the development of NETs, it is known that unhealthy lifestyle and environmental factors in general increase the risk of cancer.
Other Factors: Other factors, such as certain hormone treatments or dietary habits, may also affect the risk of NETs, but these relationships have not been fully clarified.
These risk factors do not mean that everyone will develop NETs, and many cases of NETs occur without any obvious risk factors. However, people with the risk factors mentioned above are advised to be careful and consult a physician, especially if signs or symptoms are noticed.
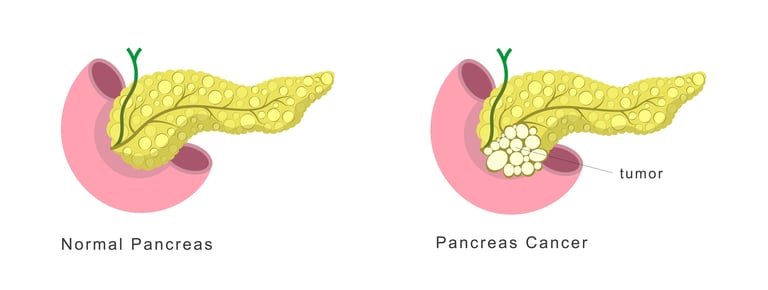
Image 1: Neuroendocrine tumors that secrete hormones may develop in the pancreatic gland.
HOW DOES IT OCCUR?
The mechanisms of development of neuroendocrine tumors (NETs) are complex and not fully understood due to the diversity of these tumors. NETs arise from cells that are part of the body's neuroendocrine system. These cells show characteristics of both the nervous and endocrine systems and secrete various hormones. The development of NETs may occur as a result of the interaction of various factors, such as genetic mutations, epigenetic changes, and environmental influences. Genetic factors play an important role, especially in certain hereditary syndromes (e.g. MEN1, von Hippel-Lindau syndrome). These mutations occur in genes that regulate cell growth and division and can lead to uncontrolled proliferation of cells and the formation of tumors. In addition, disruption of the mechanisms that regulate hormone production by neuroendocrine cells may also contribute to the development of NETs. NETs are generally slow-growing tumors, but some can be aggressive and spread quickly. The development and behavior of NETs also varies depending on the organ in which the tumor is located, the cell type, and whether the tumor produces hormones.
WHAT ARE THE SYMPTOMS?
Neuroendocrine tumors (NETs) can cause a variety of symptoms, which vary depending on the tumor's location, size, and whether it produces hormones. Some NETs may cause no symptoms, while others may cause specific symptoms.
Common findings of NETs:
Hormonal Effects: Some NETs can produce hormones or hormone-like substances, causing unique clinical syndromes. For example, pancreatic NETs can lead to conditions such as insulinoma (excessive insulin production) or gastrinoma (excessive stomach acid production).
Abdominal Pain and Digestive Problems: NETs located in the gastrointestinal tract can cause symptoms such as abdominal pain, nausea, vomiting, diarrhea, constipation and digestive disorders.
Lung Symptoms: NETs in the lung can cause symptoms such as cough, shortness of breath, and recurrent lung infections.
Flushing and Diarrhea: Some NETs cause excessive secretion of hormones such as serotonin, which can cause skin redness and flushing and diarrhea.
Changes in Blood Sugar Levels: Pancreatic NETs, like insulinoma, can lower blood sugar levels, causing hypoglycemia (low blood sugar) and related symptoms.
Weight Loss and Loss of Appetite: General symptoms such as deterioration in general health, weight loss and loss of appetite may be seen, especially in advanced stage NETs.
Sensation of Mass or Swelling: A mass or swelling may be felt in the area where the tumor is located.
Symptoms of NETs are often vague and can be confused with other common diseases. Therefore, diagnosis is often difficult and requires detailed medical evaluation. If you have such symptoms, especially if they persist for a long time or are unexplained, it is important to seek medical help.
HOW IS IT DIAGNOSED?
Neuroendocrine tumors (NETs) are usually diagnosed using a combination of various diagnostic tests and examinations. The first step is to take the patient's medical history and perform a physical examination. At this stage, symptoms, family health history, and any risk factors are taken into account. Because NETs often produce specific hormones, blood and urine tests are performed to measure the levels of these hormones. Imaging tests are also important and include ultrasonography, computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET). These tests help determine the location, size and spread of the tumor. Another method used especially for NETs is somatostatin receptor scintigraphy, which targets somatostatin receptors and shows the spread of the tumor in the body. When deemed necessary, samples of tumor tissue are taken by biopsy and examined under a microscope. This helps determine the type and grade of the tumor and guides the creation of the most appropriate treatment plan. Diagnosis of NETs can be complex and often requires an approach involving many different areas of expertise.
WHAT ARE THE PATHOLOGICAL TYPES?
Neuroendocrine tumors (NETs) are divided into several pathological types, which are classified according to the type of cell from which the tumor originates, whether it produces hormones, and other characteristics.
The main pathological types of NETs:
Gastroenteropancreatic Neuroendocrine Tumors (GEP-NETs): These tumors arise from neuroendocrine cells found throughout the digestive tract and pancreas. GEP-NETs are divided into pancreatic NETs (PNETs) and gastrointestinal NETs.
Pancreatic Neuroendocrine Tumors (PNETs): They are tumors located in the pancreas and capable of producing various hormones. There are different types such as insulinoma, gastrinoma, glucagonoma.
Gastrointestinal Neuroendocrine Tumors: NETs are found in the stomach, small intestine, appendix, colon and rectum. Carcinoid tumors are in this category.
Pulmonary Neuroendocrine Tumors: They are NETs found in the lungs and are classified as typical carcinoid, atypical carcinoid, large cell neuroendocrine carcinoma, and small cell lung cancer.
Thymic Neuroendocrine Tumors: They are rare tumors that develop in the thymus gland.
Medullary Thyroid Cancer: It is a type of NET arising from parafollicular C cells in the thyroid gland. It produces calcitonin and is often associated with MEN 2 syndrome.
Pituitary Tumors: They are tumors that develop in the pituitary gland, producing or not producing hormones.
Paraganglioma and Pheochromocytoma: These are neuroendocrine tumors that develop in the nervous system and adrenal glands, respectively. These tumors can produce hormones such as adrenaline and noradrenaline.
There are important receptors and molecular targets to focus on in neuroendocrine tumors (NETs), which play critical roles in diagnostic and therapeutic approaches. Most NETs intensely express somatostatin receptors (SSTR). The presence of these receptors can be detected by imaging methods such as somatostatin receptor scintigraphy and can determine the effectiveness of targeted therapies such as somatostatin analogs (e.g., octreotide or lanreotide). Additionally, some NETs, particularly pancreatic NETs, may have other targets such as tyrosine kinase receptors. These receptors can be targeted in treatment with tyrosine kinase inhibitors (e.g., sunitinib). Other important molecular targets include the mTOR pathway (e.g., everolimus treatment) and potentially PD-L1 and other immuno-oncological targets. Molecular characterization of NETs allows personalized approaches to the treatment of these tumors and helps determine optimal treatment strategies for patients. Determining the presence and activity of these molecular targets is done by genetic and molecular tests, and this information plays an important role in treatment planning and monitoring the course of the disease.
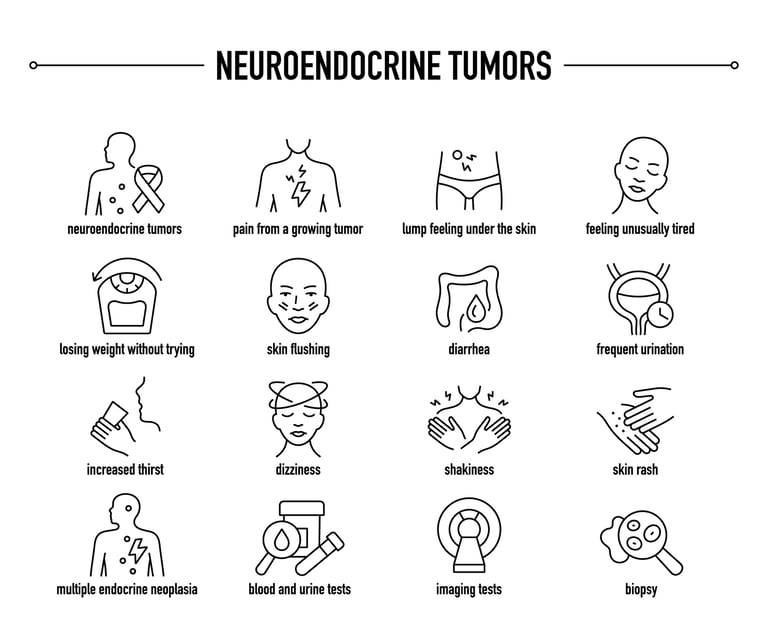
Image 2: Neuroendocrine tumors can cause complaints such as pain, skin lesions, flushing and diarrhea.
HOW IS TUMOR STAGING DONE?
Tumor staging in neuroendocrine tumors (NETs) is a system used to determine how far the cancer has progressed and spread. Staging of NETs is usually based on the size of the tumor and its spread to lymph nodes and other organs. This staging is usually based on the TNM (Tumor, Nodules, Metastasis) system:
T (Tumor) - Size and Location of the Tumor: The size and depth of the tumor at its starting point. It is classified as T1 through T4, where T1 represents the smallest and T4 represents the largest or deepest-seated tumor.
N (Lymph node) Indicates whether the cancer has spread to the lymph nodes. N0 indicates no spread to lymph nodes, N1 indicates spread to lymph nodes.
M (Metastasis)- Distant Metastasis: It shows whether the cancer has spread to other parts of the body. M0 means no distant metastasis; M1 indicates the presence of metastasis.
Staging for NETs also depends on tumor grade, which provides information about the rapidity and aggressiveness of the tumor. Grade determines how quickly tumor cells divide and how different they look from normal cells. It is classified as Grade 1 (low grade, slow growing), Grade 2 (medium grade) and Grade 3 (high grade, fast growing).
Staging of NETs is important in determining diagnosis and treatment options and is often used to evaluate the prognosis of the disease. Various imaging tests (CT, MRI, PET) and diagnostic procedures such as biopsy may be required for staging.
HOW IS TREATMENT DONE ACCORDING TO STAGES?
Treatment for neuroendocrine tumors (NETs) by stage is determined by factors such as the type of tumor, its size, its spread, and whether it produces hormones.
Commonly used approaches to treating NETs:
Early Stage NETs (Stage I and II):
Surgery: Early-stage NETs are usually treated with surgery. Its goal is to remove the tumor and affected tissue as completely as possible.
Local Treatments: For small and local tumors, local treatment methods such as radiofrequency ablation or embolization can be applied.
Locally Advanced Stage NETs (Stage III):
Surgery: If tumor spread is limited, surgical intervention may be performed.
Radiotherapy: Can be used for local control or to reduce symptoms.
Somatostatin Analogues: In hormone-producing tumors, somatostatin analogs (e.g., octreotide or lanreotide) are used to control symptoms.
Advanced Stage NETs (Stage IV):
Somatostatin Analogues: Continues for hormone production and symptom control.
Targeted Therapies: Drugs such as tyrosine kinase inhibitors (for example, sunitinib) or mTOR inhibitors (for example, everolimus) may help block the growth and spread of cancer cells.
Chemotherapy: May be used in some advanced-stage NETs, especially pancreatic NETs.
Peptide Radionuclide Receptor Therapy (PRRT): It is a treatment that carries radioactive substances to tumor cells by binding to somatostatin receptors.
Palliative Care: Palliative care is important for managing symptoms and improving quality of life in advanced-stage NETs.
A multidisciplinary approach is essential in the treatment of NETs. Experts from different disciplines such as endocrinology, gastroenterology, oncology, radiology and surgery come together to create the most appropriate treatment plan. Monitoring the disease is also important because NETs can progress slowly and require long-term monitoring. The treatment plan is personalized taking into account the patient's general health condition, the characteristics of the tumor, and the patient's preferences.
Image 3: The main treatment for neuroendocrine tumors is surgery. Systemic drugs and nuclear medicine drugs can be used in advanced neuroendocrine tumors.


WHAT ARE THE SYSTEMIC DRUGS USED IN TREATMENT?
There are a variety of medications and treatments used to treat neuroendocrine tumors (NETs). These include chemotherapies, hormonal drugs, targeted therapies (smart drugs) and immunotherapies. Here are some of these treatment options:
Chemotherapy drugs: Chemotherapy drugs used in NETs include streptozocin, 5-fluorouracil (5-FU), doxorubicin, and temozolomide. It is more commonly used in pancreatic NETs.
Somatostatin Analogues: It is used for symptom control and slowing tumor growth. Examples of these are octreotide and lanreotide. These medications help control symptoms caused by hormone-secreting NETs.
Targeted Therapies (Smart Drugs):
Tyrosine Kinase Inhibitors: Sunitinib is used in the treatment of pancreatic NETs.
mTOR Inhibitors: Everolimus is especially effective in advanced pancreatic NETs.
Peptide Radionuclide Receptor Therapy (PRRT):
Lutetium Lu 177 dotatate provides radioactive treatment by targeting somatostatin receptors.
Immunotherapies:
Immunotherapy is being investigated in the treatment of NETs, especially in advanced stages and in cases resistant to standard treatments.
Immunotherapeutic agents such as PD-1 or PD-L1 inhibitors are being studied in this field, but the use of these treatments is not yet widespread.
Each of these treatments is chosen depending on the type of tumor, its stage, and the patient's general health. Treatment planning is individualized according to the nature of the disease and the patient's needs and is usually carried out by a multidisciplinary team. The goal of treatment is to control symptoms, slow the progression of the disease, and improve the patient's quality of life.
HOW SHOULD FOLLOW-UP BE CARRIED OUT AFTER RECOVERY?
Postremission follow-up for neuroendocrine tumors (NETs) is vital to detect early risk of disease recurrence and monitor long-term health status. The follow-up process is often customized based on the type and grade of the tumor and the patient's overall health. It usually includes regular physical exams, blood tests (to check hormone levels and tumor markers), and imaging tests (ultrasonography, CT, MRI, or PET scans). In somatostatin receptor-positive NETs, specialized imaging tests such as somatostatin receptor scintigraphy can be used. Patients should inform their doctors if symptoms reoccur or change and should not interrupt their regular follow-up. In some cases, especially advanced or high-grade NETs, more frequent follow-up may be necessary. Follow-up provides a critical opportunity for early intervention in case the disease relapses or metastasizes and is also important for updating the patient's treatment plan. Post-treatment follow-up requires a multidisciplinary approach to monitor disease progression and maximize the patient's quality of life.
Legal Information
The brand name ''Onkoloji Doktorum'' has been registered by the Turkish Patent and Trademark Office.
All content on this site is for informational purposes for patients receiving cancer treatment in Türkiye. Consult your doctor for treatment planning.
All content on the site is translated from Turkish. Translation errors may be present. An oncology physician should be consulted for incomprehensible information.
All articles and images used on our website are licensed and protected by DMCA. Unauthorized use or copying is prohibited.
Contact
Assoc. Prof. Dr. İzzet Doğan
Internal Medicine and Medical Oncology Specialist
Acıbadem Healthcare Group
Atakent ve Bakırköy Hospitals
Call for an Appointment: +90 444 55 44
Acıbadem Atakent Hospital
Telephone: +90 212 404 44 44
Acıbadem Bakırköy Hospital
Telephone: +90 212 414 44 44