Malignant Melanoma
21.03.2025
MMALIGN MELANOMA DIAGNOSIS AND TREATMENT
Malignant melanoma is a serious type of cancer that arises from pigment cells called melanocytes in the skin. This cancer develops due to DNA damage, especially from exposure of the skin to UV rays. While malignant melanoma can be treated when diagnosed early, it can quickly metastasize and spread to other organs if diagnosed late or left untreated. This spread complicates treatment and poses serious health risks for the patient. Therefore, it is important to consult a physician if new moles or changes in existing moles are noticed on the skin. Risk factors for malignant melanoma include light skin color, family history of melanoma, history of sunburn, and a high number of atypical moles. Prevention and early diagnosis play a vital role in controlling this disease.
WHAT ARE THE RISK FACTORS?
There are many risk factors that affect the development of malignant melanoma. Some of these factors are:
Skin Type: People with fair skin, light/green eyes, and blonde/red hair color have a higher risk of melanoma.
Sun Exposure: Exposure to intense UV light, especially that causing sunburn, increases the risk of melanoma.
Sunburns: Severe sunburns, especially in childhood, can increase the risk of melanoma in the future.
Family History of Melanoma: Having a history of melanoma in a family member increases the risk.
Skin Cancer History: People who have previously had skin cancer have a higher risk of developing melanoma.
Atypical Moles: Numerous and/or irregular, large moles (atypical nevi) increase the risk of melanoma.
Lifetime Sun Exposure: The risk of melanoma may increase especially in people who work outdoors or those who sunbathe frequently.
Solarium and UV Lamps: Exposure to artificial UV light, especially use of solariums at young ages, increases the risk of melanoma.
Genetic Factors: Certain genetic mutations are among the factors that increase the risk of melanoma.
Weakness of the Immune System: The risk of melanoma may increase in people who have diseases or use medications that suppress the immune system.
The presence of these risk factors increases the chance of developing melanoma, but the presence of any of these factors does not necessarily mean that melanoma will develop. Regular skin checks and preventive measures play an important role in reducing the risk of melanoma.
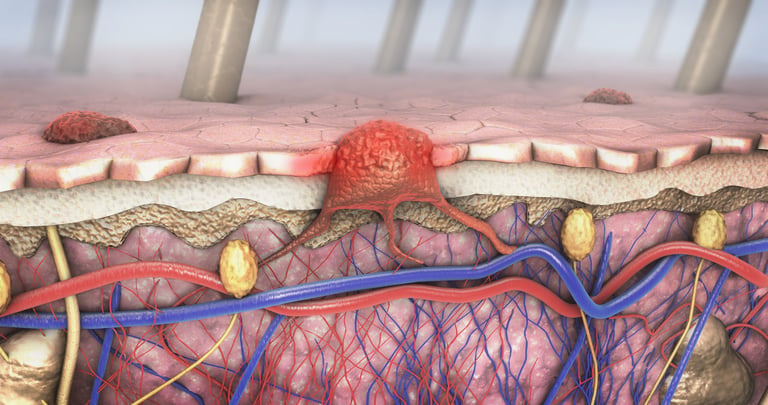
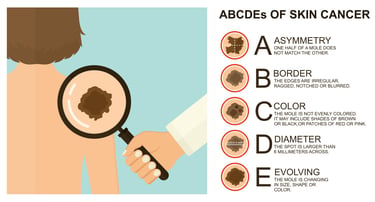
Image 1: Although there are different types of cancer that develop in the skin, the worst type is malignant melanoma.


HOW IT OCCURS?
Malignant melanoma is a type of cancer that occurs in melanocytes, the pigment-producing cells of the skin. The development of this cancer usually begins with DNA damage caused by UV rays. UV light causes mutations in the DNA of melanocytes, and these mutations cause the cells to divide and proliferate in an uncontrolled and abnormal way. Normally, the body can recognize and destroy damaged cells, but sometimes these mechanisms fail or mutations disable these control mechanisms. Thus, damaged melanocytes begin to spread, forming a tumor. Genetic predisposition also plays an important role in the development of malignant melanoma; Individuals with a family history of melanoma have a higher risk of developing this type of cancer. Additionally, environmental factors such as atypical moles on the skin and sun exposure also increase the risk of developing melanoma. This complex process is the subject of ongoing research to understand why some individuals develop melanoma and others do not.
WHAT ARE THE SYMPTOMS?
Signs and symptoms of malignant melanoma usually appear as visible changes in the skin. Some of these symptoms include:
Change in Moles: Changes in the shape, size or color of existing moles. Melanomas often begin with the change of existing moles, but they can also appear as new moles.
Asymmetry: While healthy moles are usually symmetrical, melanomas can be asymmetrical. If one half of the mole looks different from the other, this could be a warning sign.
Edges: The edges of melanomas are often irregular, jagged or discontinuous.
Color: The color of the mole may be uneven and may include shades of brown, black, pink, red, white or blue.
Printing: Melanomas usually measure more than 6 mm in diameter, but they can be smaller.
Development and Change: Development or rapid change in the size, shape or color of the mole may occur over time.
Itching or Pain: Melanomas may be itchy or painful.
Bleeding or CrustingMelanomas may bleed, crust over, or peel off at the top.
If any of these symptoms are noticed, it is important to consult a dermatologist. While melanoma can be treated when diagnosed early, it can become more difficult and complex to treat when it progresses to advanced stages. Therefore, it is important to have regular skin examinations and pay attention to risk factors.
HOW IS IT DIAGNOSED?
Diagnosis of malignant melanoma typically begins with a careful examination of the skin by a dermatologist. The dermatologist evaluates the size, shape, color and other characteristics of moles and other lesions on the skin. For suspicious-looking lesions, a special magnifying glass called dermatoscopy is used to examine the microscopic details of the lesion. If melanoma is suspected, a biopsy is performed for definitive diagnosis. During biopsy, all or part of the lesion is surgically removed and sent to the pathology laboratory for examination under a microscope. The pathologist determines the presence and type of cancer cells by performing detailed examinations on the sample. Additional imaging tests (for example, MRI, CT, or PET scans) may be used to support or stage the diagnosis when necessary. This stepwise approach is critical in the accurate and early diagnosis of melanoma.
WHAT ARE THE PATHOLOGICAL TYPES?
Malignant melanoma can be classified according to its main pathological types, and each of these types shows different characteristics and prognostic values.
The most common types of melanoma are:
Superficial Spreading Melanoma: It is the most common type of melanoma. It usually occurs in young and middle-aged adults. Melanoma slowly spreads and expands on the skin surface.
Nodular Melanoma: This type of melanoma can grow more aggressively and spread quickly into the deeper skin layers. Nodular melanomas often appear dark or black, but they can also be colorless.
Lentigo Maligna Melanoma: It is usually seen in the elderly and on skin areas that are heavily exposed to the sun. It is more common in areas such as the face and neck. It begins as a lesion that grows slowly over many years.
Acral Melanoma: It is seen on the hands and feet, especially under the nails and in the palms. This type of melanoma is more common in ethnically darker-skinned people.
Desmoplastic Melanoma: It is a rare type and usually occurs in the face and neck area. It is characterized by fibrosis (tissue hardening) and can be difficult to diagnose.
Mucosal Melanoma: It develops on the mucosal surfaces of the body (mouth, nose, genital area, etc.). This type of melanoma is rare and may be more aggressive than other types.
Ocular Melanoma: It is a type of melanoma that develops in the eye. This type of melanoma is located in the internal structure of the eye, especially the choroid.
Each type of melanoma displays specific histological features and growth patterns, and treatment options are determined depending on this pathological type and stage of melanoma. Especially in rare types, an expert team approach is important for accurate diagnosis and appropriate treatment.
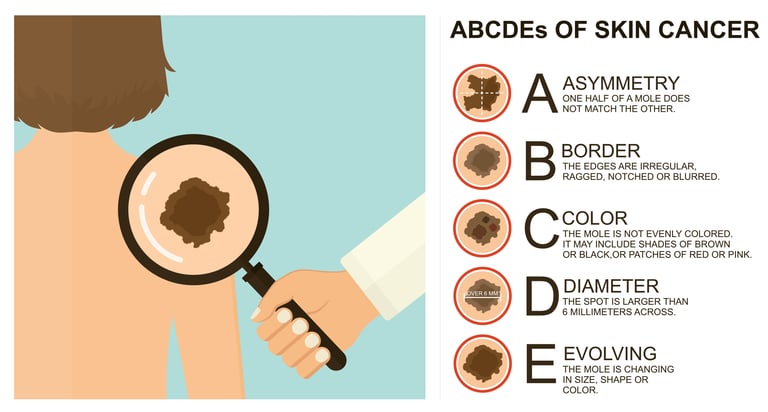
Image 2: In suspicious skin lesions, features such as asymmetry, border irregularity, color change, large size and diameter growth should be monitored in terms of cancer development.
WHAT ARE THE RECEPTORS TO LOOK AT?
In malignant melanoma, some important receptors and molecular markers to look at to understand the biological behavior of the tumor and its response to treatment are:
BRAF Mutations: These are genetic mutations seen in approximately 40-60% of melanoma patients. In particular, the BRAF V600E mutation is important in the use of certain targeted therapies.
c-KIT Mutations: These are mutations seen especially in melanomas exposed to mucosal, acral and chronic sun damage. These mutations may affect the response to some targeted therapies.
NRAS Mutations: It is another important mutation found in approximately 15-20% of melanoma patients and may affect treatment options.
GNAQ and GNA11 Mutations: These mutations are especially important in ocular melanoma patients and are among potential treatment targets.
PD-1/PD-L1 Ekspresyonu: Programmed cell death receptor-1 (PD-1) and its ligand (PD-L1) may influence the response to immunotherapy in melanoma. High expression of PD-1 or PD-L1 may indicate better response to immunotherapies.
Microsatellite İnstability (MSI) ve Tumor Mutational Burden (TMB): High MSI and/or TMB have been associated with response to immunotherapy in melanoma.
These receptors and molecular markers play an important role in the diagnosis and treatment of melanoma. Genetic profiling of the tumor is increasingly used to understand the nature of the disease and determine the most effective treatment strategies. However, such tests require expertise in performing and interpreting their results and are often requested in specific clinical situations.
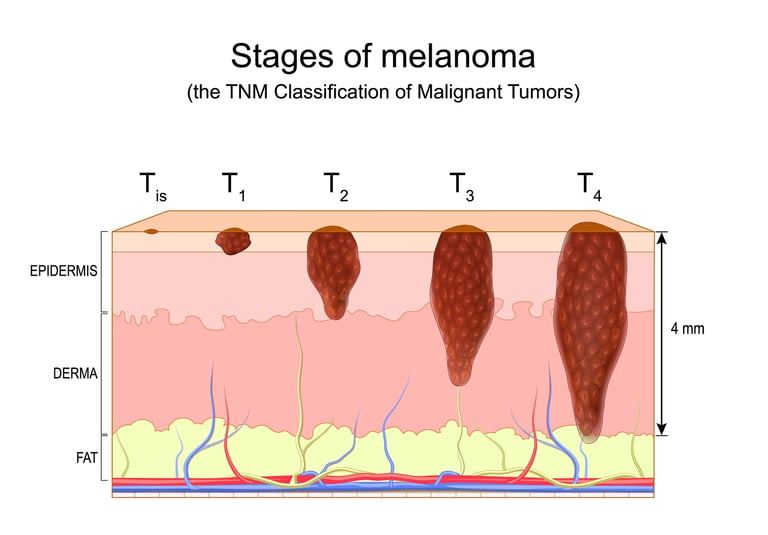
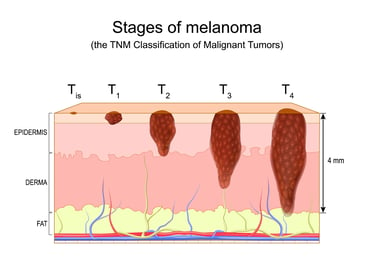
HOW IS TUMOR STAGING DONE?
Tumor staging of malignant melanoma is a system used to determine the extent and severity of cancer. This staging is done according to the depth of the melanoma, its spread throughout the body and other characteristics. Staging is important for treatment planning and prognosis prediction. Staging of melanoma is based on:
Thickness of the Tumor (Breslow Thickness): Measures how deep the melanoma has gone into the skin. As thickness increases, melanoma is thought to be more aggressive and has a poor prognosis.
Presence of Ulceration: Disruption of the upper layer of the tumor (ulceration) is a poor prognostic sign.
From Myth to Oran: The division (mitosis) rate of tumor cells. A higher mitotic rate indicates a more aggressive tumor.
Lymph Node Involvement: It determines whether the tumor has spread to nearby lymph nodes. Lymph node involvement indicates that the disease is at a more advanced stage.
Metastasis: It means the spread of the tumor to other organs or body parts. The presence of metastasis indicates stage IV (most advanced stage) melanoma.
Melanoma is divided into stages, usually numbered 0 to IV:
Euro 0 (in situ melanoma):The tumor is found only in the top skin layer (epidermis).
Evre I-II: It is determined according to the thickness of the tumor and the presence of ulceration. There is no spread to lymph nodes.
Stage III: The tumor has spread to nearby lymph nodes.
Stage IV: The tumor has metastasized to distant organs.
This staging plays a critical role in determining the melanoma treatment plan and patient follow-up. Each stage of the disease differs in terms of prognosis and treatment options. Various tests and evaluations, especially biopsy, imaging techniques, and physical examination, are used for staging.
Image 3: Malignant melanoma is divided into stages according to the degree of superficial involvement in the skin, the presence of ulcers, lymph node involvement, and spread to distant organs.
HOW IS TREATMENT DONE ACCORDING TO STAGES?
Treatment of malignant melanoma varies depending on the stage of the cancer. Treatment approaches for each stage are as follows:
Stage 0 (In Situ Melanoma)
Surgery: Removing (excising) the entire tumor. It is generally a superficial and local process.
Stage I and II (Early Stage Melanoma)
Surgery: The tumor must be removed with extensive surgery. In high-risk cases, a biopsy of nearby lymph nodes (sentinel lymph node biopsy) may be performed.
Adjuvant Therapy: In high-risk patients, preventive treatments may be recommended to reduce the risk of spread.
Stage III (Regional Advanced Stage Melanoma)
Surgery: Removal of affected lymph nodes.
Systemic Therapies: Immunotherapy (e.g. PD-1 inhibitors, CTLA-4 inhibitors), targeted therapies (BRAF and MEK inhibitors, if suitable mutations are present) and chemotherapy.
Radiation Therapy: In some cases, it may be used to destroy any remaining cancer cells after surgery.
Evre IV (Metastatic Melanoma)
Systemic Therapies: Immunotherapy, targeted therapies, sometimes chemotherapy. These treatments aim to control the spread of the disease and prolong life.
Palliative Care: Supportive treatments to relieve symptoms and improve quality of life.
Surgery and Radiation: In certain cases, it may be applied for symptom control or local control.
General Approaches
Clinical Trials: At all stages, participating in clinical trials testing new treatments may be an option.
Regular Follow-Up and Monitoring: Regular follow-up and monitoring is important against the risk of melanoma recurrence.
Personalized treatment approaches are important in melanoma treatment. Factors such as the patient's general health condition, tumor characteristics and molecular profile may affect treatment options. It is necessary to collaborate with oncology specialists to determine the most appropriate treatment plan for each patient.
WHAT ARE THE SYSTEMIC DRUGS USED IN TREATMENT?
There are various treatment methods used in malignant melanoma. These include chemotherapy, targeted therapies (smart drugs) and immunotherapies. Examples of each type of treatment are as follows:
Chemotherapy pills
Dacarbazine (DTIC): One of the most commonly used chemotherapy drugs.
Temozolomide: It is especially used in patients with brain metastases.
Platinum-based medications: Drugs such as cisplatin or carboplatin are sometimes used to treat melanoma.
Targeted Therapies (Smart Drugs)
BRAF Inhibitors: Vemurafenib and dabrafenib are used in patients with BRAF mutations.
MEK Inhibitors: Trametinib and cobimetinib. It is often used together with BRAF inhibitors.
c-KIT Inhibitors: Imatinib may be effective in some melanomas carrying the c-KIT mutation.
Immunotherapies
PD-1 Inhibitors: Pembrolizumab and nivolumab activate the immune system by targeting the PD-1/PD-L1 pathway.
CTLA-4 Inhibitor: Ipilimumab activates the immune system, helping it fight against tumor cells.
Interleukin-2 (IL-2): At high doses, it can be a powerful form of immunotherapy.
These drugs are used in personalized treatment approaches according to the molecular and genetic characteristics of melanoma. Treatment options are determined based on molecular profiling of the tumor and the patient's general health status. Additionally, due to rapid advances in melanoma treatment and the constant development of new treatment options, it is important to stay in regular contact with oncology specialists to obtain the most up-to-date information in this field
HOW SHOULD FOLLOW-UP BE CARRIED OUT AFTER RECOVERY?
Follow-up after treatment for malignant melanoma is critical to detect early recurrence of the disease and manage long-term health problems. Post-healing follow-up usually includes the following steps: Regular skin examinations, monthly skin checks by the patient, and comprehensive skin examinations by a dermatologist every 3-6 months are important. These examinations help detect new or changing skin lesions early. Additionally, for particularly high-risk patients, full-body scanning may be recommended at regular intervals using imaging tests such as PET, CT, or MRI. These scans are done to check if melanoma has recurred in other parts of the body. Patients should also maintain protective measures such as limiting sun exposure, using sunscreens with a high protection factor, and paying attention to risk factors. Emotional and psychological support is also important in the post-treatment period, because cancer treatment and recovery can be mentally and emotionally challenging.
Legal Information
The brand name ''Onkoloji Doktorum'' has been registered by the Turkish Patent and Trademark Office.
All content on this site is for informational purposes for patients receiving cancer treatment in Türkiye. Consult your doctor for treatment planning.
All content on the site is translated from Turkish. Translation errors may be present. An oncology physician should be consulted for incomprehensible information.
All articles and images used on our website are licensed and protected by DMCA. Unauthorized use or copying is prohibited.
Contact
Assoc. Prof. Dr. İzzet Doğan
Internal Medicine and Medical Oncology Specialist
Acıbadem Healthcare Group
Atakent ve Bakırköy Hospitals
Call for an Appointment: +90 444 55 44
Acıbadem Atakent Hospital
Telephone: +90 212 404 44 44
Acıbadem Bakırköy Hospital
Telephone: +90 212 414 44 44