Gestational Trophoblastic Disease
21.03.2025
GESTATIONAL TROPHOBLASTIC DISEASE DIAGNOSIS AND TREATMENT
Gestational Trophoblastic Disease (GTD) refers to a group of rare diseases that occur as a result of abnormal growth and proliferation of trophoblastic cells during pregnancy. This disease occurs due to abnormal development and invasion of cells on the placenta of pregnancy. The importance of GTD is that it tends to grow rapidly and has invasive properties. Therefore, early diagnosis and treatment is necessary. GTD can present with symptoms such as vaginal bleeding, pelvic pain, and high beta-hCG (human chorionic gonadotropin) levels. Risk factors may include age, previous pregnancy history, and family history. Accurate diagnosis and effective treatment of GTD is vital to preserve the patient's health. Therefore, early diagnosis and appropriate treatment of this disease is a condition that should be followed carefully during pregnancy.
WHAT ARE THE RISK FACTORS?
Risk factors for Gestational Trophoblastic Disease (GTD) may include:
Previous Gestational Trophoblastic Disease: People who have had GTD before are at risk of recurrent GTD.
Age: GTD is generally more common in younger and older pregnancies. Pregnant women over the age of 40 may be especially at risk.
Previous Pregnancy History: Those who have experienced complications in previous pregnancies or problems such as molar pregnancy may be at risk of GTD.
Family History: People with a family history of GTD may be at risk of contracting this disease.
Early or Late Pregnancies: Early or late pregnancies may increase the risk of GTD.
First Pregnancy: Women with their first pregnancy may have a higher risk of GTD compared to other pregnancies.
Nutritional Factors: Malnutrition, low folic acid intake or vitamin deficiencies may increase the risk of GTD.
Smoking: Smoking during pregnancy may be one of the factors that can increase the risk of GTD.
GTD risk factors can vary from person to person, and the presence of these factors can affect a person's likelihood of developing GTD. However, these factors do not always explain the exact causes of the disease, and the risk of developing GTD is low in every pregnant woman. Therefore, even if a person has these factors, regular prenatal follow-up and compliance with doctor's recommendations are important.
Image 1: Gestational trophoblastic disease is a rare disease that occurs as a result of abnormal growth and proliferation of trophoblastic cells during pregnancy.
HOW DOES IT OCCUR?
The developmental mechanisms of Gestational Trophoblastic Disease (GTD) are complex and not yet fully understood. But basically, GTD occurs as a result of abnormal growth and proliferation of trophoblastic cells. Trophoblastic cells are the cells that normally form the placenta and settle on the inner surface of the uterus during pregnancy. In GTD, uncontrolled growth and invasion of these cells is observed. These abnormal trophoblastic cells adhere tightly to the lining of the uterus, replacing normal tissues and can penetrate blood vessels. This process leads to vaginal bleeding, high beta-hCG levels, and other symptoms. Although the developmental mechanisms have not been fully elucidated, research on the molecular origins of this disease continues.
WHAT ARE THE SYMPTOMS?
Signs and symptoms of Gestational Trophoblastic Disease (GTD) may include:
Vaginal Bleeding: GTD usually presents with abnormal vaginal bleeding. This bleeding may occur during or after pregnancy.
Pelvic Pain: Patients may experience pain or discomfort in the pelvic area. This pain may occur due to abnormal growth and invasion in the uterus.
High Beta-hCG Levels: Beta-hCG (human chorionic gonadotropin) levels in the blood of GTD patients may be much higher than normal. Beta-hCG is an important marker in the diagnosis of the disease.
Hyperemesis Gravidarum: In rare cases, patients with GTD may experience severe nausea and vomiting, a condition called hyperemesis gravidarum.
Symptoms of Gestational Trophoblastic Disease may vary from person to person and may differ depending on the type of disease.
HOW IS IT DIAGNOSED?
Gestational Trophoblastic Disease (GTD) is diagnosed by symptoms, physical examination and laboratory tests. The first step is usually based on the presence of symptoms, especially if there are symptoms such as abnormal vaginal bleeding and high beta-hCG (human chorionic gonadotropin) levels. Physical examination is important to evaluate abnormalities in the pelvic area. Laboratory tests include measuring beta-hCG levels, and high levels raise suspicion of GTD. Ultrasonography is used to visually examine the internal structure of the uterus and can detect signs that indicate abnormalities. Definitive diagnosis is made by histopathological examination. Pathology may involve examining tissue samples taken during a biopsy or curettage. All these tests are important to diagnose GTD and determine the type of disease.
WHAT ARE THE PATHOLOGICAL TYPES?
The pathological types of Gestational Trophoblastic Disease (GTD) are:
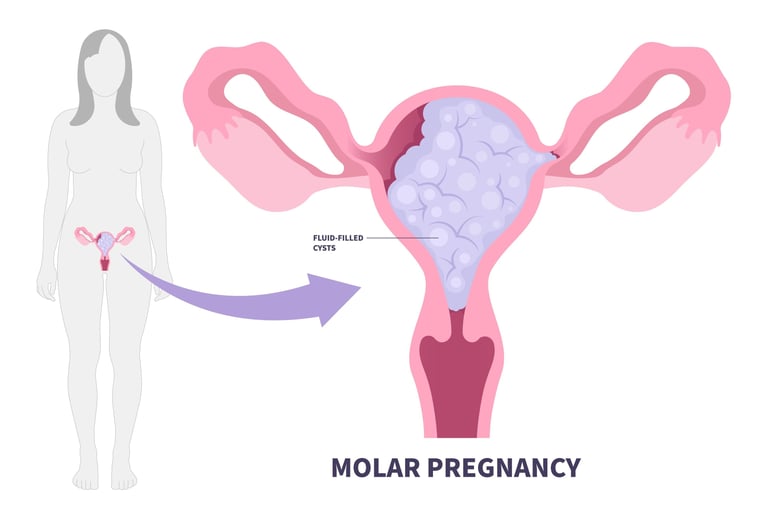
Hydatidiform Mole (Molar Pregnancy): Hydatidiform mole refers to a condition in which the placenta grows abnormally and trophoblastic cells proliferate at an abnormal rate. This condition results in a pregnancy in which normal fetal development stops and the fetus does not develop. Hydatidiform mole may include two subtypes: complete and partial.
Invasive Hydatidiform Mole: This type of GTD is a more aggressive form of hydatidiform mole. Trophoblastic cells can penetrate the lining of the uterus more deeply and invasively. This situation carries the risk of spreading to surrounding tissues.
Choriocarcinoma: Choriocarcinoma is a rarer and more aggressive form of GTD. This type of GTD refers to a condition in which trophoblastic cells become cancerous and tend to grow rapidly and metastasize (spread to other organs).
Placental Cytotrophoblastic Tumors: This type of GTD refers to a condition in which cytotrophoblastic cells grow abnormally and the placenta is abnormal.
Pathological types of Gestational Trophoblastic Disease may affect treatment and follow-up, considering the nature of the disease and its mode of spread. Therefore, correct diagnosis and determination of the pathological type are important in determining the treatment approach.
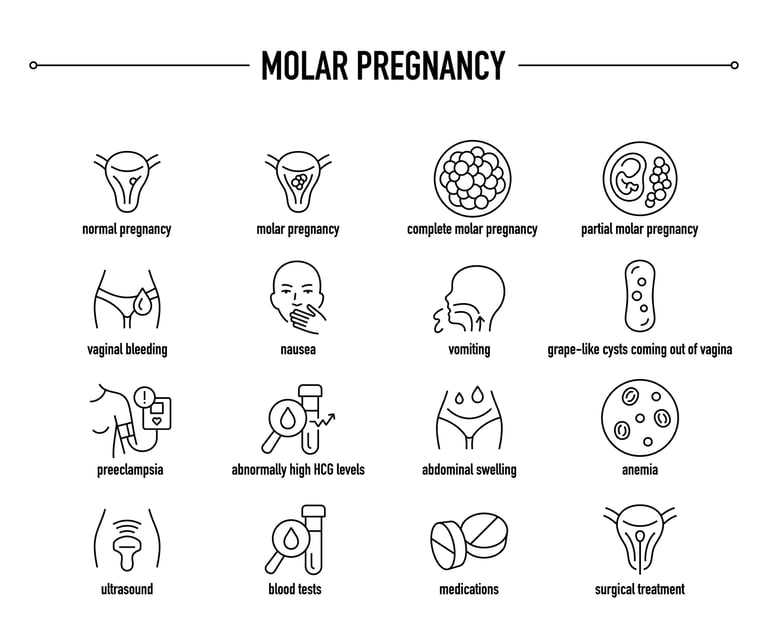
Image 2: Gestational trophoblastic disease complaints such as vaginal bleeding, abdominal pain, nausea and vomiting may occur during pregnancy.
HOW IS TUMOR STAGING DONE?
Tumor staging of Gestational Trophoblastic Disease (GTD) is used to determine the extent and severity of the disease. Staging is important in determining which areas the disease has spread and treatment options. Tumor staging of GTD is done as follows:
Stage I: GTD remains confined within the uterus and has not spread to nearby tissues.
Stage II: GTD may have spread outside the uterus, but is usually limited to the pelvic organs.
Stage III: GTD can spread from the pelvic organs to more distant areas, especially the lungs.
Stage IV: GTD has spread to distant organs, for example, the liver, brain, or other distant sites.
Additionally, tumor staging can be further determined by the patient's beta-hCG (human chorionic gonadotropin) levels and imaging studies. Tumor staging plays an important role in assessing the extent of disease spread, creating a treatment plan, and predicting the patient's prognosis. Treatment is determined according to the patient's tumor stage and general health condition.
HOW IS TREATMENT DONE ACCORDING TO STAGES?
Gestational Trophoblastic Disease (GTD) may require different treatment approaches depending on the stages. Here are the treatment approaches of GTD according to stages:
Stage I GTD Treatment: In this stage, when GTD is limited, it is generally low risk and is usually treated with surgery. Curettage may be performed to clean the uterine contents. The patient's beta-hCG levels are then closely monitored. Monitoring continues until levels normalize.
Stage II GTD Treatment: If stage II GTD has spread to the pelvic organs, surgical intervention may be required. This surgical procedure may involve removing the patient's uterus. Additionally, beta-hCG levels and follow-up imaging studies are used to guide treatment.
Stage III GTD Treatment: If GTD has spread to areas outside the pelvic area (for example, to the lungs), chemotherapy treatment may be considered. Combination chemotherapy treatment is a common approach. Beta-hCG levels and imaging studies are used to evaluate response to treatment.
Stage IV GTD Treatment: When GTD has spread to distant organs (for example, the liver or brain), intensive chemotherapy may often be an option. The treatment plan is determined depending on the patient's general health condition and the degree of spread of the tumor.
Treatment plans may be different for each patient and are evaluated individually by a specialist oncologist. After treatment, the patient's recovery process is monitored and monitored with beta-hCG levels and imaging studies. If treatment is successful, patients usually continue to have regular follow-up exams for several years.
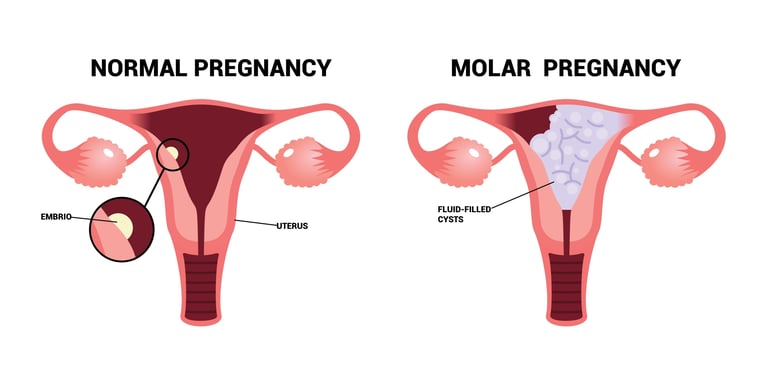
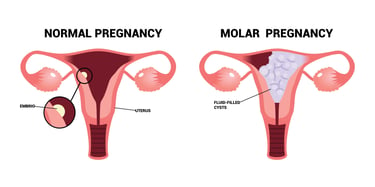
Image 3: Molar pregnancy (grape pregnancy) is the most common cause of gestational trophoblastic diseases.
WHAT ARE THE SYSTEMIC DRUGS USED IN TREATMENT?
Chemotherapy, smart drug therapies and immunotherapies used in the treatment of Gestational Trophoblastic Disease (GTD) may include:
Chemotherapy drugs:
Methotrexate: Methotrexate is a chemotherapy drug commonly used in the treatment of GTD.
Dactinomycin: Dactinomycin (actinomycin-D) is an effective chemotherapy agent in the treatment of GTD.
Etoposide: Etoposide is another chemotherapy drug that can be used in the advanced stages of GTD.
Bleomycin: Bleomycin is another chemotherapy drug that can be used in the treatment of GTD.
Immunotherapies: As immunotherapy, pembrolizumab, nivolumab and avelumab may be considered as a treatment option.
Treatment options may vary depending on the patient's tumor stage, type, and general health condition. Therefore, it is evaluated and determined individually by a specialist oncologist. Any treatment plan must be tailored to the patient's specific condition and needs.
HOW SHOULD FOLLOW-UP BE DONE AFTER RECOVERY?
Follow-up after Gestational Trophoblastic Disease (GTD) treatment is of great importance to monitor the patient's recovery process and evaluate the risk of recurrence of the disease. Post-recovery follow-up usually includes regular measurement of beta-hCG (human chorionic gonadotropin) levels. Beta-hCG levels should normalize after treatment. Additionally, imaging studies (for example, computed tomography or ultrasonography) examine the body for any signs of recurrent lesions or tumors. Follow-up period may vary depending on the patient's response to treatment, the stage of the disease and risk factors. Doctors monitor patients' health closely and evaluate for signs of recurrence or complications. Patients should attend regular follow-up examinations, follow their doctor's recommendations, and report any abnormalities or symptoms immediately. In this way, early diagnosis and treatment may be possible in case of recurrence of GTD.
Legal Information
The brand name ''Onkoloji Doktorum'' has been registered by the Turkish Patent and Trademark Office.
All content on this site is for informational purposes for patients receiving cancer treatment in Türkiye. Consult your doctor for treatment planning.
All content on the site is translated from Turkish. Translation errors may be present. An oncology physician should be consulted for incomprehensible information.
All articles and images used on our website are licensed and protected by DMCA. Unauthorized use or copying is prohibited.
Contact
Assoc. Prof. Dr. İzzet Doğan
Internal Medicine and Medical Oncology Specialist
Acıbadem Healthcare Group
Atakent ve Bakırköy Hospitals
Call for an Appointment: +90 444 55 44
Acıbadem Atakent Hospital
Telephone: +90 212 404 44 44
Acıbadem Bakırköy Hospital
Telephone: +90 212 414 44 44