Esophageal Cancer
21.03.2025
ESOPHAGUS CANCER DIAGNOSIS AND TREATMENT
Esophagus Cancer is a type of cancer that occurs in the organ called the esophagus or esophagus. The esophagus is a tube-shaped organ located between the mouth and stomach and allows food to pass into the stomach. This type of cancer usually occurs as a result of abnormal, uncontrolled growth and proliferation of cells of the esophagus. Esophageal cancer is a serious health problem worldwide and treatment can be challenging because it is usually detected in advanced stages. The importance of esophageal cancer is linked to the fact that it usually does not cause symptoms in the early stages and causes more pronounced symptoms as it progresses. This type of cancer can present with symptoms such as difficulty swallowing, weight loss, chest pain, and heartburn. Risk factors may include smoking, excessive alcohol consumption, chronic reflux, obesity and genetic factors. The importance of early diagnosis can increase the effectiveness of treatment options and increase the chances of survival. Therefore, it is important to have regular health checks when symptoms appear or risk factors are present. Treatment may often include surgery, chemotherapy and radiotherapy. The treatment plan for esophageal cancer is determined depending on the general health of the patient, the size of the tumor and its spread. Therefore, it is vital for individuals to be conscious, try to minimize risk factors and pay attention to regular health checks for early diagnosis and effective treatment of serious health problems such as esophageal cancer.
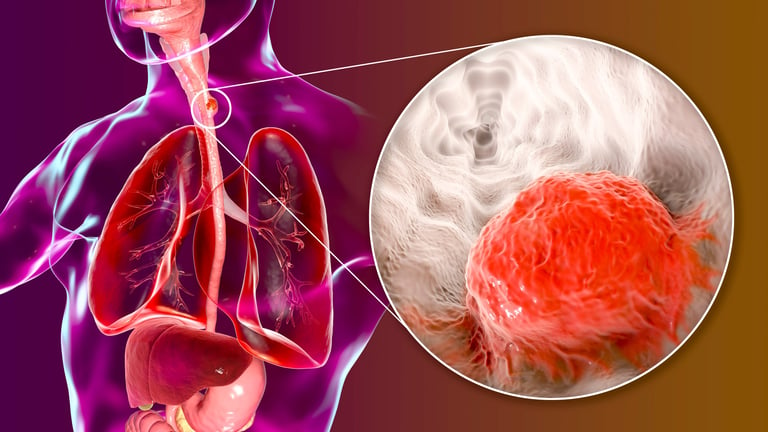
Image 1: Many complaints such as burning in the chest, weight loss and difficulty swallowing can be observed in esophageal cancer.
WHAT ARE THE RISK FACTORS?
Esophageal cancer risk factors include various conditions and lifestyle choices that can increase the likelihood of developing cancer.
Some of the risk factors for esophageal cancer are:
Tobacco Use: Smoking or chewing tobacco is one of the most important risk factors for esophageal cancer.
Excessive Alcohol Consumption: Regular and excessive alcohol consumption, especially when combined with tobacco use, increases the risk of esophageal cancer.
Gastroesophageal Reflux Disease (GERD): Prolonged or uncontrolled acid reflux can lead to a condition called Barrett's esophagus.
Barrett's Esophagus: An advanced complication of GERD, this condition causes abnormal cell changes in the esophageal lining and increases the risk of cancer.
Obesity: A high body mass index (BMI), especially fat around the rib cage and abdomen, may increase the risk of esophageal cancer.
Damage to the Esophagus: Past damage to the esophagus, such as chemical burns, may increase the risk of esophageal cancer.
Hot Drinks and Foods: Consuming very hot drinks and foods can damage the esophageal lining and increase the risk of cancer.
Some Diet Factors: Dietary factors such as inadequate fruit and vegetable consumption, excessive consumption of processed meats and foods containing nitrates/nitrites may increase the risk.
Family History: Family members with a history of esophageal cancer may increase the risk of developing cancer.
Some Medical Conditions: Some medical conditions related to the esophagus, such as achalasia, may increase the risk.
The presence of these risk factors does not necessarily mean that they will lead to esophageal cancer, but they may increase the risk. Therefore, it is important for people with risk factors to have regular medical check-ups and, if necessary, screening for early diagnosis.
HOW DOES IT OCCUR?
Esophageal cancer is characterized by DNA damage in the cells of the esophagus and subsequent abnormal cell growth. This type of cancer usually begins in the squamous cells lining the inner surface of the esophagus or in the gland cells in the lower part where it meets the stomach. Risk factors include tobacco and alcohol use, gastroesophageal reflux disease (GERD), Barrett's esophagus, obesity, and certain dietary habits. These factors can cause DNA damage in cells, leading to mutations. These mutations in esophageal cells cause cells to divide and proliferate uncontrollably, disrupting normal cell death mechanisms and ultimately forming tumors. Over time, these tumors can spread (metastasize) to surrounding tissues and other organs, leading to the progression of esophageal cancer and serious health problems. This process often takes years and may be asymptomatic in the early stages, making diagnosis and treatment difficult.
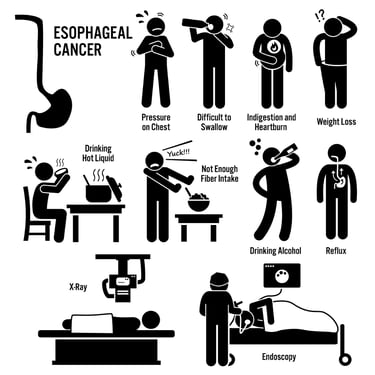
WHAT ARE THE SYMPTOMS?
Esophageal cancer is a type of cancer that begins in the cells of the esophagus and usually begins in the cells on the surface of the esophagus. Symptoms of esophageal cancer may include:
Difficulty in Swallowing (Dysphagia): Difficulty or discomfort when swallowing is one of the most common symptoms of esophageal cancer. As cancer progresses, it may become more difficult to swallow solid food due to narrowing of the esophagus.
Weight Loss: Unexplained weight loss may occur as a result of inadequate nutrition, especially due to difficulty swallowing.
Chest Pain or Discomfort: Pain, burning, or discomfort may occur behind the breastbone.
Hoarseness or Cough: Esophageal cancer can put pressure on the nerves of the larynx and cause hoarseness or a chronic cough.
Pain or Discomfort After Eating: Pain or discomfort in the chest or stomach may occur after eating.
Heartburn and Acid Reflux: Frequent heartburn or acid reflux symptoms may occur.
These symptoms can occur with many different conditions besides esophageal cancer, so medical evaluation and tests are important for an accurate diagnosis. If you are experiencing any of these symptoms, it is important to consult a healthcare professional.
Image 2: The diagnosis of esophageal cancer is made by pathological examination of the biopsy piece taken by endoscopy.
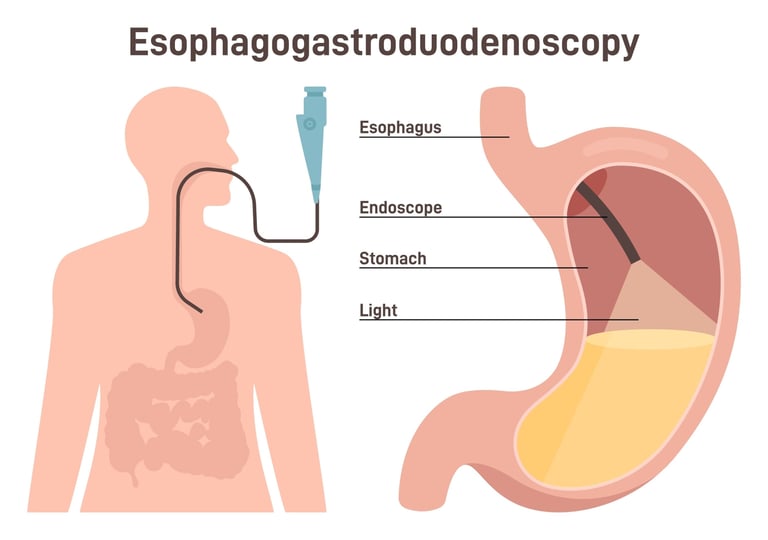
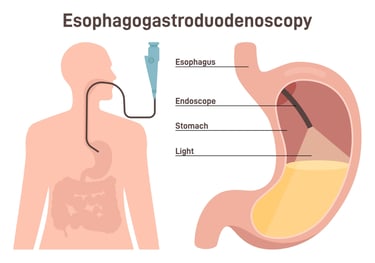
HOW IS IT DIAGNOSED
Diagnosis of esophageal cancer usually begins after symptoms appear and involves a series of diagnostic tests and procedures. The first step is to take the patient's medical history and perform a physical examination. The most common diagnostic tool, upper gastrointestinal endoscopy (upper GI endoscopy), is then used. During this procedure, doctors make direct observation by inserting a thin, flexible tube (endoscope) with a camera and light source into the patient's esophagus. If a suspicious area is seen, a biopsy is performed and tissue samples are taken and examined under a microscope. Additionally, imaging tests such as computed tomography (CT) scans, magnetic resonance imaging (MRI), and positron emission tomography (PET) scans may be used to determine the spread and stage of the cancer. These tests help evaluate the size of the cancer, its spread in the esophagus and surrounding tissues, and detect possible lymph nodes or distant organ metastases. All this information is critical for an accurate assessment of the patient's condition and the creation of an appropriate treatment plan.
WHAT ARE THE PATHOLOGICAL TYPES?
Esophageal cancer is divided into different pathological types based on the main cell type and histological features. The two main types are:
Squamous Cell Carcinoma: It is the most common type of esophageal cancer and begins in the flat cells (squamous cells) lining the inside of the esophagus. This type of cancer usually occurs in the middle and upper parts of the esophagus and is closely associated with tobacco use and alcohol consumption.
Adenocarcinoma: It is more common in the lower part of the esophagus and originates from gland cells in the area where it meets the stomach. This type of cancer is often associated with gastroesophageal reflux disease (GERD) and Barrett's esophagus. It is more common than squamous cell carcinoma in Western countries, especially the United States.
Apart from these, other rarer types of esophageal cancer include:
Melanoma
Leiomyosarcoma
Lymphoma
These types make up a very small percentage of esophageal cancers and usually require more specific treatments. The pathological type of esophageal cancer is an important factor in determining how the cancer is treated and its prognosis. Each type of cancer shows different characteristics at the cellular level, which causes treatment options and approaches to differ. During the diagnosis and treatment process of esophageal cancer, various receptors and molecular markers related to cell growth, division and spread of cancer are examined. Priorities for these studies include Epidermal Growth Factor Receptor (EGFR), HER2/neu (Human Epidermal Growth Factor Receptor 2), Vascular Endothelial Growth Factor (VEGF) and the p53 tumor suppressor gene. Additionally, markers such as Ki-67, which indicates cell proliferation, and PD-L1 (Programmed Cell Death Ligand 1), which can determine the response to immunotherapies, are also important. These receptors and markers play critical roles in assessing the aggressiveness of esophageal cancer, its potential to spread, and responses to various treatments. This information is vital for managing the disease and personalizing treatment options and may vary depending on each patient's condition. Therefore, treatment planning of patients diagnosed with esophageal cancer requires careful evaluation of these molecular and genetic factors
HOW IS TUMOR STAGING DONE?
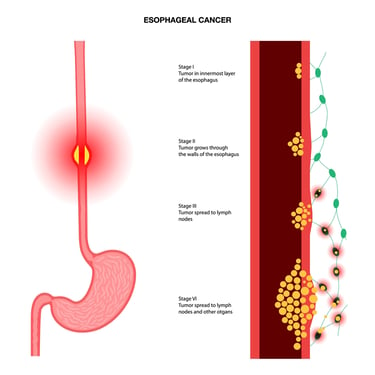
Tumor staging in esophageal cancer is a process used to determine how far the cancer has spread. This process evaluates the size of the tumor, its spread to surrounding tissues, and its possibility of metastasizing to lymph nodes or other organs. Staging is based on the TNM system:
T (Tumor): T category determines which layers of the esophagus the main tumor has spread to and the size of the tumor. There are different stages from T1 to T4, T1 refers to the smallest and least spread tumors, and T4 refers to tumors that have spread outside the esophagus and involve neighboring structures.
N (Lymph Node): N category indicates whether the cancer has spread to nearby lymph nodes. N0 means there are no cancer cells in the lymph nodes; N1, N2 and N3 indicate increasing degrees of lymph node involvement.
M (Metastasis): Category M evaluates whether the cancer has spread to other organs outside the esophagus. M0 means no distant metastasis; M1 indicates the presence of metastasis.
Based on this TNM classification, esophageal cancer is usually divided into stages 0 through IV. While Stage 0 refers to the situation where the cancer is superficial and has not spread to the deep layers of the esophagus, Stage IV represents the most advanced stage in which the cancer has metastasized to distant organs.
Diagnostic methods used for tumor staging include endoscopy, biopsy, computed tomography (CT) scan, positron emission tomography (PET) scan, and magnetic resonance imaging (MRI). These tests help evaluate the tumor's characteristics, location and spread in detail. Staging plays a critical role in treatment planning and determining prognosis.
HOW IS TREATMENT DONE ACCORDING TO STAGES?
Treatment of esophageal cancer varies depending on the stage of the cancer, the patient's general health and other individual factors. Treatment approaches for each stage are generally as follows:
Stage 0 (High Grade Dysplasia or Early Cancer)
Endoscopic interventions: It is the process of removing cancerous tissue with minimally invasive procedures such as endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD).
Radiotherapy: In some cases, it can be used to destroy cancerous tissue.
Early Stage (Stage I and II)
Surgery: A surgical procedure called esophagectomy is used to remove the tumor and affected lymph nodes.
Chemotherapy and Radiotherapy: Can be used in pre-surgical (neoadjuvant) or post-surgical (adjuvant) treatment. These treatments are administered to improve surgical outcomes and reduce the risk of cancer spreading.
Advanced Stage (Stage III and sometimes II)
Chemoradiotherapy: Chemotherapy and radiotherapy are used in combination to destroy cancer cells and prepare them for surgery.
Surgery: In stage III, esophagectomy may be performed in some cases, but is usually evaluated after chemoradiation.
Metastatic Cancer (Stage IV)
Systemic Chemotherapy: Used to control cancer and relieve symptoms.
Targeted therapies and Immunotherapy: In some cases, treatments directed at specific genetic mutations or molecular targets may be applied.
Palliative Care: Supportive treatments to manage pain and other symptoms.
General Approach
Nutritional support and rehabilitation: Esophageal cancer and its treatments can affect the ability to eat; Therefore, nutritional support is important.
Regular follow-up and monitoring: Regular follow-up after treatment is important in detecting recurrence or progression of cancer at an early stage.
Since each patient's condition is different, treatment plans should be prepared individually. Oncologists, surgeons, radiation oncologists, gastroenterologists and other health professionals work with a multidisciplinary approach in determining treatment options for esophageal cancer.
Image 3: Esophageal cancer is divided into stages according to involvement of the esophageal layers, lymph node involvement, and spread to distant organs.
WHAT ARE SYSTEMIC TREATMENTS?
Chemotherapy, targeted therapies (smart drugs), immunotherapies and hormonal treatments used in the treatment of esophageal cancer vary depending on the type and stage of the cancer and the general health status of the patient.
Chemotherapy Drugs
Cisplatin: Often used together with radiation therapy.
5-Fluorouracil (5-FU): It is given in combination with cisplatin.
Docetaxel: Can be combined with other chemotherapeutic agents.
Oxaliplatin: Can be combined with 5-FU or capecitabine.
Carboplatin: Sometimes used with other agents.
Paclitaxel: It is used especially in squamous cell carcinoma.
Targeted Therapies (Smart Drugs)
Trastuzumab: Used in HER2 positive esophageal adenocarcinomas.
Ramucirumab: Targets the vascular endothelial growth factor (VEGF) receptor.
Immunotherapies
Pembrolizumab: Used in PD-L1 positive advanced or metastatic squamous cell esophageal cancer.
Nivolumab: It is a PD-1 inhibitor used especially in advanced stage esophageal cancers.
Combined Treatment Approaches
Most often, these agents are used in combination to treat esophageal cancer. For example, chemotherapy and radiotherapy may be given together in neoadjuvant or adjuvant therapy.
Treatment options used in esophageal cancer vary depending on the biological characteristics of the cancer, the general health status of the patient and the stage of the cancer. Each treatment method should be evaluated individually, taking into account side effects and the patient's response to treatment. Treatment plans and drug choices should be made individually by an oncologist.
HOW SHOULD FOLLOW-UP BE DONE AFTER RECOVERY?
Follow-up after recovery from esophageal cancer is critical to detect early disease recurrence, manage the long-term effects of treatment, and monitor the patient's overall health. This follow-up process usually includes regular medical exams, endoscopic check-ups, and imaging tests (for example, computed tomography or PET scans). For the first few years, these checks are usually done every 3-6 months because the risk of recurrence is highest during this period. Thereafter, follow-up intervals may be extended annually. In addition, patients' nutritional status, swallowing difficulties and other quality of life issues are evaluated regularly. If necessary, patients are supported by a multidisciplinary healthcare team such as dietitians, physiotherapists and psychological support services. Patients are also made aware of any new signs or symptoms so they can quickly seek medical help in the event of a possible recurrence or complication. This process is personalized based on the patient's health status and adjusted to each patient's needs.
Legal Information
The brand name ''Onkoloji Doktorum'' has been registered by the Turkish Patent and Trademark Office.
All content on this site is for informational purposes for patients receiving cancer treatment in Türkiye. Consult your doctor for treatment planning.
All content on the site is translated from Turkish. Translation errors may be present. An oncology physician should be consulted for incomprehensible information.
All articles and images used on our website are licensed and protected by DMCA. Unauthorized use or copying is prohibited.
Contact
Assoc. Prof. Dr. İzzet Doğan
Internal Medicine and Medical Oncology Specialist
Acıbadem Healthcare Group
Atakent ve Bakırköy Hospitals
Call for an Appointment: +90 444 55 44
Acıbadem Atakent Hospital
Telephone: +90 212 404 44 44
Acıbadem Bakırköy Hospital
Telephone: +90 212 414 44 44