Bile Tract Cancer
21.03.2025
BILE DUCT CANCER DIAGNOSIS AND TREATMENT


Bile tract cancer is a rare but serious type of cancer that arises from the cells lining the inside of the bile ducts. This type of cancer is commonly known as cholangiocarcinoma and can affect parts of the bile ducts inside (intrahepatic) or outside (extrahepatic) the liver. Bile duct cancer can be difficult to treat, especially when diagnosed in advanced stages, because this type of cancer often progresses silently without noticeable symptoms. When diagnosed at an early stage, surgical removal of the tumor may be the most effective treatment method. However, in most cases the cancer has spread by the time it is diagnosed, and treatment options are limited. The importance of biliary tract cancer is increasing due to its rarity and difficulty in diagnosis and treatment. This emphasizes awareness of this type of cancer and the importance of early diagnosis. Understanding risk factors, developing early diagnosis methods and creating effective treatment strategies are the main focuses of research in this field.
WHAT ARE THE RISK FACTORS?
Bile duct cancer is a rare type of cancer and may be associated with various risk factors. The most important among these factors are:
Primary sclerosing cholangitis (PSC): This chronic liver disease significantly increases the risk of developing biliary tract cancer.
Chronic Bile Duct Infections: Some parasitic infections, especially common in Southeast Asia (for example, Opisthorchis viverrini and Clonorchis sinensis), may increase the risk of biliary tract cancer.
Gallstones and Gallbladder Diseases: Long-term presence of gallstones and other gallbladder diseases may increase the risk of biliary tract cancer.
Congenital Bile Duct Anomalies: Congenital biliary tract abnormalities may increase the risk of biliary tract cancer.
Family History and Genetic Predisposition: In families with a history of bile duct cancer, the risk of developing cancer may be higher.
Age and Gender: Bile duct cancer is generally more common in older individuals and men.
Chronic Hepatitis and Liver Cirrhosis: Chronic hepatitis B or C infection and liver cirrhosis may increase the risk of biliary tract cancer.
Chemical Exposure: Long-term exposure to certain industrial chemicals (for example, radiological contrast agents such as thorotrast) may increase the risk of biliary tract cancer.
Smoking: There is evidence that smoking increases the risk of biliary tract cancer.
These risk factors may increase the likelihood of developing biliary tract cancer, but may differ in each individual. Regular health checks and, if necessary, screening tests are recommended for early diagnosis in individuals with risk factors.
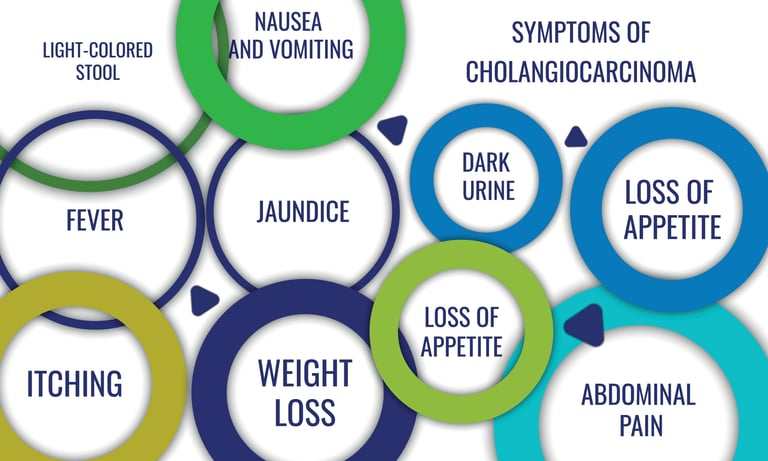
Image 1: Many complaints such as loss of appetite, nausea, vomiting and jaundice may be observed in bile duct cancer.

HOW DOES IT OCCUR?
Bile tract cancer is a type of cancer that usually arises from the cells lining the inner surface of the bile ducts and develops as a result of genetic and molecular changes in these cells. At the beginning of cancer development, DNA damage occurs in the epithelial cells of the bile ducts. This damage can result from a variety of environmental and genetic factors. For example, chronic inflammation, gallstones, bile duct diseases such as primary sclerosing cholangitis (PSC), or some parasitic infections can trigger cancer development by causing oxidative stress and DNA damage in cells. These damages to DNA can lead to genetic mutations that cause cells to divide uncontrollably and cause tumor formation. Additionally, in this process, the normal programmed death mechanisms of cells (apoptosis) are disrupted and the survival of abnormal cells is ensured. In later stages, these abnormal cells can proliferate, block the bile ducts and spread to surrounding tissues. The development of bile duct cancer is the result of such a complex series of biological changes, and these changes present important targets in the diagnosis and treatment of cancer.
WHAT ARE THE SYMPTOMS?
Bile duct cancer may not cause symptoms, especially in the initial stages, but as it progresses, various findings may occur. These symptoms may vary from patient to patient, but the most common findings are:
Jaundice (Icterus): Bile duct cancer can block the flow of bile, causing yellowing of the skin and whites of the eyes.
Stomach achePain can usually be felt on the right side of the upper abdomen, and this pain can also spread to the back and shoulders.
Weight Loss: Unexplained and unintentional weight loss is a common symptom of many types of cancer, including biliary tract cancer.
Anorexia: A decrease in appetite may be observed in the later stages.
Dark Urine and Light Colored Stool: Obstruction in bile flow can cause urine to darken and stool to be lighter in color than normal.
Itching: A general itching of the skin may be associated with the accumulation of bile salts under the skin.
Fever and Chills: In some cases, fever and chills may be seen as signs of infection.
Abdominal Bloating: There may be gas, bloating or discomfort in the abdominal area.
Although each of these symptoms is not a definitive sign of biliary tract cancer, they should be taken into consideration, especially in individuals with risk factors. When any alarming symptoms are noticed, it is important to consult a healthcare professional for early diagnosis and treatment. Since bile duct cancer is often diagnosed in advanced stages, early identification of such symptoms can be vital.
HOW IS IT DIAGNOSED?
Diagnosis of bile duct cancer can often be difficult because it may not present obvious symptoms in the early stages. The diagnostic process begins with the patient's symptoms, medical history, and physical examination findings. As a first step, blood tests are performed; These tests check the function of the liver and bile ducts and may indicate abnormalities. Liver function tests and tumor markers (e.g., CA 19-9) are especially important. Imaging tests are an important part of diagnosis, and methods such as ultrasound, computed tomography (CT), magnetic resonance cholangiopancreatography (MRCP), and endoscopic retrograde cholangiopancreatography (ERCP) may be used. These imaging tests can identify tumors in the bile ducts, narrowings, and obstructions to bile flow. If necessary, the presence and type of the tumor can be confirmed by taking a biopsy from the bile ducts. The diagnostic process may also require additional testing to determine the extent and stage of the disease.
WHAT ARE THE PATHOLOGICAL TYPES?
Biliary tract cancer is mainly known as cholangiocarcinoma, and this type of cancer is divided into several pathological types that can develop in different parts of the bile ducts. These types are:
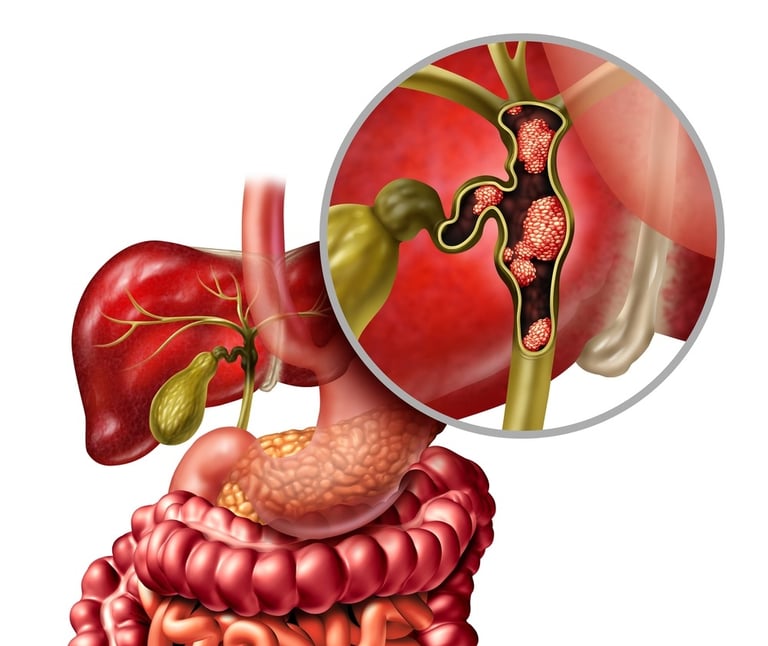
Intrahepatic Cholangiocarcinoma: It develops in the bile ducts inside the liver. Intrahepatic cholangiocarcinoma is a less common type of bile duct cancer and is often considered different from hepatocellular carcinoma.
Extrahepatic cholangiocarcinoma: It develops in the bile ducts outside the liver and is divided into two subcategories:
Perihilar (Hilar) Cholangiocarcinoma: It develops in the hilus, the area where the bile ducts exit the liver. This type is also known as "Klatskin tumor" and is the most common type of biliary tract cancer.
Distal Cholangiocarcinoma: It develops in the lower parts of the bile ducts, especially in areas close to the pancreas.
Gallbladder Cancer: Although not technically classified as biliary tract cancer, gallbladder cancer is also associated with the bile ducts and exhibits similar risk factors and pathological features.
Each pathological type of cancer varies in terms of spread, treatment options and prognosis. For example, while intrahepatic cholangiocarcinoma generally has a more aggressive course, tumors in the hilus region may be more suitable for surgical intervention. Therefore, accurate identification of biliary tract cancer is important in determining the appropriate treatment strategy. There are some receptors and molecular markers that should be taken into consideration in the treatment and diagnosis of bile duct cancer. Vascular Endothelial Growth Factor (VEGF) and its receptors play a role in the growth of cancer by helping the tumor form new blood vessels. KRAS mutation attracts attention as a genetic change that is frequently seen in biliary tract cancers and may affect the response to treatment. Immunologically, positivity for Programmed Cell Death Protein 1 (PD-1) and its ligand PD-L1 are used to determine response to immunotherapies. Analysis of these receptors and markers can provide important information about the biology of biliary tract cancer and help identify targeted treatment options. Therefore, determining these molecular features in the treatment of biliary tract cancer is of great importance in terms of patient-specific treatment planning and increasing the effectiveness of the treatment.
Image 2: Bile tract cancer can develop in the bile ducts inside or outside the liver.
HOW IS TUMOR STAGING DONE?
Tumor staging in bile duct cancer is a process used to determine the extent of spread and severity of the cancer. This staging is done based on factors such as the size of the tumor, its local spread, and its spread to lymph nodes and other organs. The staging process includes these steps:
Tumor Size and Local Spread (T):The size and degree of spread of the tumor in the bile ducts are determined. It shows whether the tumor affects only the bile ducts or has spread to surrounding tissues.
Lymph Nodes (N): It is examined whether the cancer has spread to the lymph nodes. Affected lymph nodes are important in terms of the spread of the disease and treatment options.
Metastasis (M): It is evaluated whether the cancer has spread outside the bile ducts, especially to distant organs (such as liver, lung, bone).
Various imaging modalities are used for this staging, such as ultrasound, computed tomography (CT), magnetic resonance imaging (MRI), and sometimes positron emission tomography (PET) scans. If necessary, tissue samples taken during biopsy or surgery may also contribute to staging. Among the staging systems used for bile duct cancer, the TNM system (Tumor, Nodule, Metastasis) and the AJCC (American Cancer Society) cancer staging system are common. These systems stage cancer by taking into account the size of the tumor, its spread to lymph nodes, and metastasis. Staging is critical for planning treatment of biliary tract cancer and assessing the patient's prognosis. The most appropriate treatment approach (surgery, radiotherapy, chemotherapy, targeted therapy or immunotherapy) is determined according to the patient's stage.
HOW IS TREATMENT DONE ACCORDING TO TUMOR STAGES?
Treatment of bile duct cancer is determined according to the stage of the disease and different treatment approaches can be applied for each stage:
Early Stage (Stage I and II): In early stage bile duct cancer, surgery is the most common treatment option. The goal of surgery is to remove all of the cancerous tissue. If the tumor is in the gallbladder, the gallbladder may need to be removed. If the tumor is in the bile ducts, the tumor as well as surrounding tissues and, if necessary, lymph nodes are also removed.
Middle Stage (Stage III): At this stage, the cancer may have spread to surrounding tissues but is still considered localized. Surgery may still be an option, but may require more extensive intervention. In addition to surgery or if surgery is not possible, radiotherapy and/or chemotherapy may be included in the treatment plan.
Advanced Stage (Stage IV): In the advanced stage, biliary tract cancer has metastasized to distant organs. The focus of treatment at this stage is usually to improve the patient's quality of life and keep symptoms under control. Surgery is usually not an option. Radiotherapy, chemotherapy and palliative care are used to improve the patient's condition and control pain.
New treatment approaches such as targeted therapies and immunotherapy can also be evaluated in treatment planning, especially in cases where the tumor displays certain genetic features or molecular targets. A multidisciplinary approach is essential in the treatment of bile duct cancer, and treatment decisions are often made by a team consisting of medical oncologists, surgeons, radiation oncologists and other oncological specialties. The patient's general health condition, the specific characteristics of the cancer, and the response to treatment play an important role in determining the treatment plan.
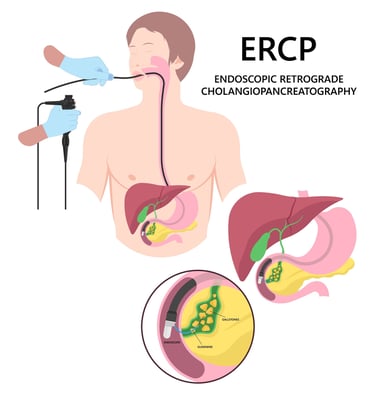
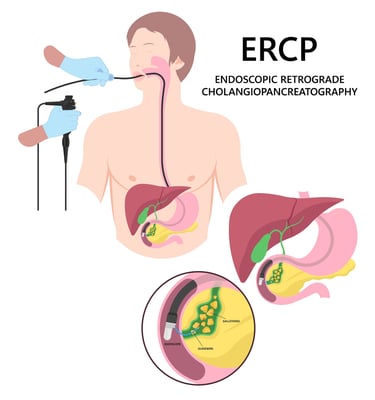
Image 3: Advanced jaundice due to obstruction in the bile ducts can be treated with the ERCP method.
WHAT ARE THE DRUGS USED IN TREATMENT?
Various treatment methods used in biliary tract cancer include chemotherapies, targeted (smart) drug therapies, and immunotherapies. These treatments can be listed as follows:
Chemotherapy Drugs:
Gemcitabine: A chemotherapy drug commonly used in biliary tract cancers.
Cisplatin: When used with gemcitabine, it may be effective in the treatment of biliary tract cancer.
5-Fluorouracil (5-FU): In some cases, it is used in the treatment of biliary tract cancer.
Oxaliplatin: Can be used in combination with other chemotherapy drugs.
Targeted (Smart) Drug Therapies:
Lenvatinib, pralsetinib, entrectinib: These drugs may be effective in biliary tract cancers with mutations such as NTRK and RET mutation.
Trastuzumab: Can be used in HER2 positive biliary tract cancers.
Immunotherapies:
Nivolumab: It is a PD-1 inhibitor usually used in patients with metastatic bile duct cancer.
Pembrolizumab: It is an immunotherapy drug that acts on the PD-1 pathway and can be used especially in biliary tract cancers with certain genetic features.
Treatment options for bile duct cancer vary depending on the characteristics of the patient's cancer, general health status, and previous treatments. Additionally, understanding the molecular and genetic profile of cancer plays an important role in the selection of these treatments. Therefore, biliary tract cancer treatment should be carried out with a multidisciplinary approach and within the framework of a personalized treatment plan.
HOW SHOULD FOLLOW-UP BE DONE AFTER RECOVERY?
Follow-up after recovery from biliary tract cancer is critical to detect early disease recurrence and monitor the patient's overall health status. Generally, monitoring is more frequent during the first few years after treatment, during which time a check may occur every 3-6 months. Follow-up may include regular physical exams, liver function tests, and blood tests such as tumor markers (for example, CA 19-9). Imaging tests, such as ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI), are important to evaluate whether the cancer has recurred. Additionally, patients are recommended to make lifestyle changes, follow a healthy diet, and exercise regularly. Follow-up plans are personalized based on patients' symptoms and overall health, and immediate medical attention is encouraged in case of any new symptoms or concerns. Psychological and social support is also important to manage the long-term effects of bile duct cancer treatment and improve patients' quality of life. This holistic approach helps patients achieve the best results in their recovery process.
Legal Information
The brand name ''Onkoloji Doktorum'' has been registered by the Turkish Patent and Trademark Office.
All content on this site is for informational purposes for patients receiving cancer treatment in Türkiye. Consult your doctor for treatment planning.
All content on the site is translated from Turkish. Translation errors may be present. An oncology physician should be consulted for incomprehensible information.
All articles and images used on our website are licensed and protected by DMCA. Unauthorized use or copying is prohibited.
Contact
Assoc. Prof. Dr. İzzet Doğan
Internal Medicine and Medical Oncology Specialist
Acıbadem Healthcare Group
Atakent ve Bakırköy Hospitals
Call for an Appointment: +90 444 55 44
Acıbadem Atakent Hospital
Telephone: +90 212 404 44 44
Acıbadem Bakırköy Hospital
Telephone: +90 212 414 44 44